Interhospital Transfer: Transfer Processes and Patient Outcomes





Though often undertaken to provide patients with specialized care, interhospital transfer (IHT) is associated with worse outcomes for select patients. Certain aspects of the transfer process have been suggested as contributors to these outcomes. We performed a retrospective cohort study including patients ≥ 18 years who underwent IHT to a tertiary care hospital between January 2005 and September 2013. We examined the association between “weekend” transfer, “nighttime” transfer, “time delay” between transfer acceptance and arrival, and admission team “busyness” on the day of transfer, and patient outcomes, including transfer to the intensive care unit (ICU) within 48 hours and 30-day mortality. We utilized multivariable logistic regression models, adjusting for patient characteristics. Secondary analyses examined detailed timing of transfer and evaluated 30-day mortality stratified by service of transfer. Among the 24,352 patients who underwent IHT, the nighttime transfer was associated with increased adjusted odds of ICU transfer (odds ratio [OR] 1.54; 95% CI 1.38, 1.72) and 30-day mortality (OR 1.16; 95% CI 1.01, 1.35). Secondary analyses confirmed the association between nighttime transfer and ICU transfer throughout the week and demonstrated that Sunday (and trend towards Friday) night transfers had increased 30-day mortality, as compared with Monday daytime transfer. Stratified analyses demonstrated a significant association between transfer characteristics and adjusted odds of 30-day mortality among cardiothoracic and gastrointestinal surgical service transfers. Our findings suggest high acuity patients have worse outcomes during off-peak times of transfer and during times of high care team workload. Further study is needed to identify underlying reasons to explain these associations and devise potential solutions.
© 2019 Society of Hospital Medicine
Outcomes
Outcomes included transfer to the intensive care unit (ICU) within 48 hours of arrival and 30-day mortality from date of index admission.5,6
Patient Characteristics
Covariates for adjustment included: patient age, sex, race, Elixhauser comorbidity score,11 Diagnosis-Related Group (DRG)-weight, insurance status, year of admission, number of preadmission medications, and service of admission.
Statistical Analyses
We used descriptive statistics to display baseline characteristics and performed a series of univariable and multivariable logistic regression models to obtain the adjusted odds of each transfer process characteristic on each outcome, adjusting for all covariates (proc logistic, SAS Statistical Software, Cary, North Carolina). For analyses of ICU transfer within 48 hours of arrival, all patients initially admitted to the ICU at time of transfer were excluded.
In the secondary analyses, we used a combined day-of-week and time-of-day variable (ie, Monday day, Monday evening, Monday night, Tuesday day, and so on, with Monday day as the reference group) to obtain a more detailed evaluation of timing of transfer on patient outcomes. We also performed stratified analyses to evaluate each transfer process characteristic on adjusted odds of 30-day mortality stratified by service of admission (ie, at the time of transfer to BWH), adjusting for all covariates. For all analyses, two-sided P values < .05 were considered significant.
RESULTS
Overall, 24,352 patients met our inclusion criteria and underwent IHT, of whom 2,174 (8.9%) died within 30 days. Of the 22,910 transferred patients originally admitted to a non-ICU service, 5,464 (23.8%) underwent ICU transfer within 48 hours of arrival. Cohort characteristics are shown in Table 1.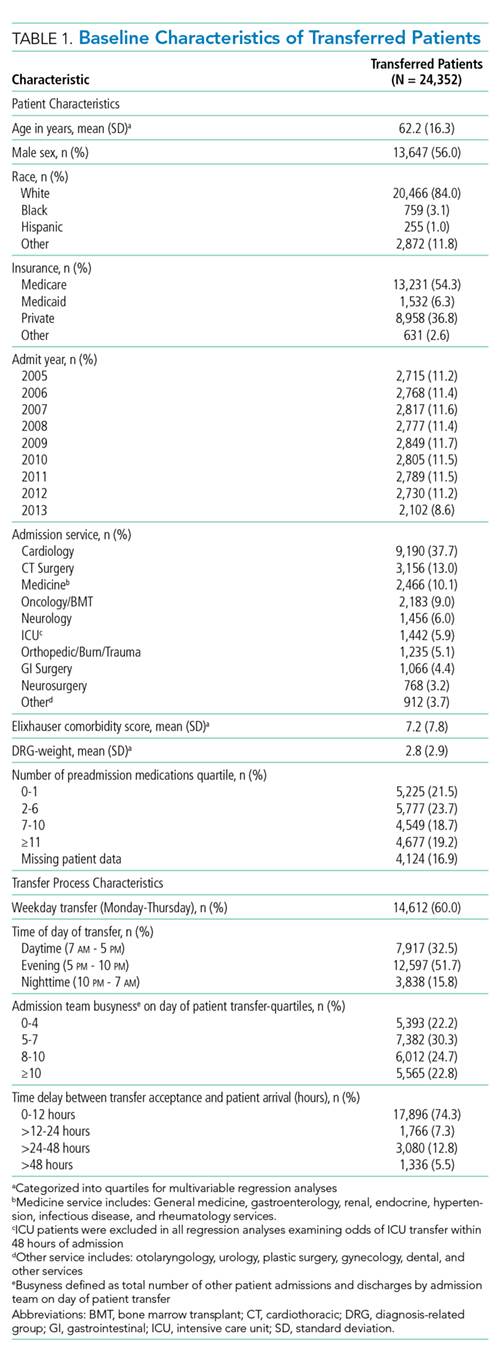
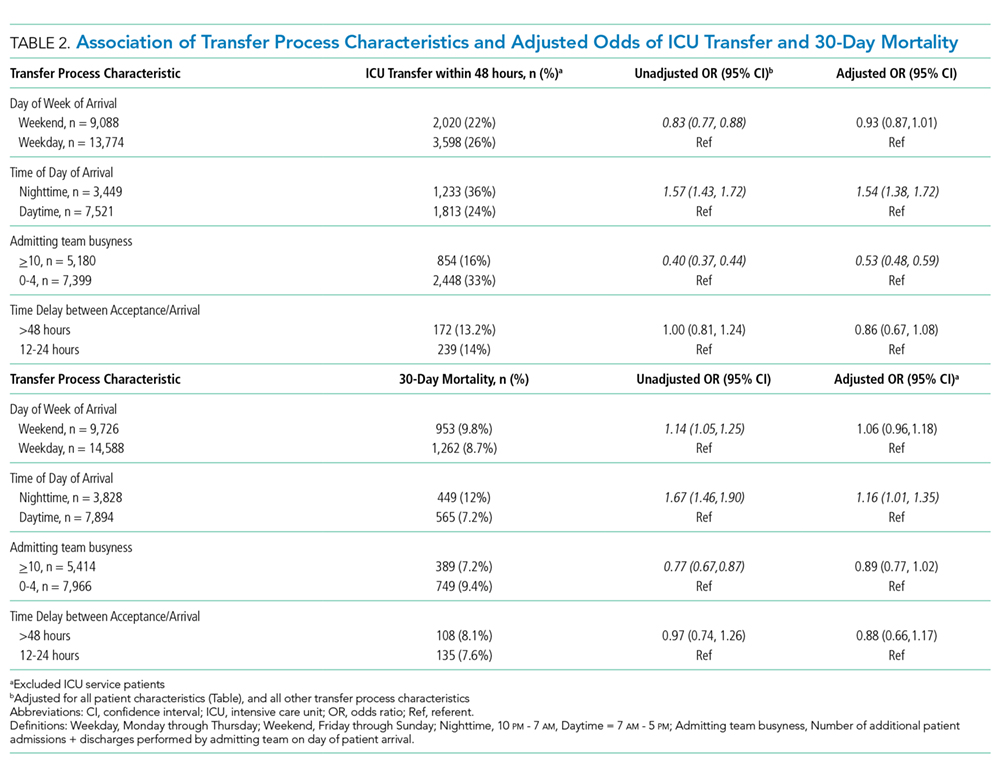
Multivariable regression analyses demonstrated no significant association between weekend (versus weekday) transfer or increased time delay between patient acceptance and arrival (>48 hours) and adjusted odds of ICU transfer within 48 hours or 30-day mortality. However, they did demonstrate that nighttime (versus daytime) transfer was associated with greater adjusted odds of both ICU transfer and 30-day mortality. Increased admitting team busyness was associated with lower adjusted odds of ICU transfer but was not significantly associated with adjusted odds of 30-day mortality (Table 2). As expected, decreased time delay between patient acceptance and arrival (0-12 hours) was associated with increased adjusted odds of both ICU transfer (adjusted OR 2.68; 95% CI 2.29, 3.15) and 30-day mortality (adjusted OR 1.25; 95% CI 1.03, 1.53) compared with 12-24 hours (results not shown). Time delay >48 hours was not associated with either outcome.
Regression analyses with the combined day/time variable demonstrated that compared with Monday daytime transfer, Sunday night transfer was significantly associated with increased adjusted odds of 30-day mortality, and Friday night transfer was associated with a trend toward increased 30-day mortality (adjusted OR [aOR] 1.88; 95% CI 1.25, 2.82, and aOR 1.43; 95% CI 0.99, 2.06, respectively). We also found that all nighttime transfers (ie, Monday through Sunday night) were associated with increased adjusted odds of ICU transfer within 48 hours (as compared with Monday daytime transfer). Other days/time analyses were not significant.
Univariable and multivariable analyses stratified by service were performed (Appendix). Multivariable stratified analyses demonstrated that weekend transfer, nighttime transfer, and increased admitting team busyness were associated with increased adjusted odds of 30-day mortality among cardiothoracic (CT) and gastrointestinal (GI) surgical service patients. Increased admitting team busyness was also associated with increased mortality among ICU service patients but was associated with decreased mortality among cardiology service patients. An increased time delay between patient acceptance and arrival was associated with decreased mortality among CT and GI surgical service patients (Figure; Appendix). Other adjusted stratified outcomes were not significant.