Impact of Pharmacist-led Discharge Counseling on Hospital Readmission and Emergency Department Visits: A Systematic Review and Meta-analysis





BACKGROUND: Transitions of care can contribute to medication errors and other adverse drug events.
PURPOSE: The aim of this study was to evaluate the impact of pharmacist-led discharge counseling on hospital readmission and emergency department visits through a systematic review and meta-analysis.
DATA SOURCES: Electronic searches were performed in PubMed, Scopus, and DOAJ (Directory of Open Access Journals), along with a manual search (July 2017). PROSPERO registration no. CRD42017068444.
STUDY SELECTION: Two independent reviewers performed all the steps of the systematic review process (screening of titles and abstracts, full-text appraisal, data extraction, and quality assessment), with contributions from a third researcher. We included randomized controlled trials (RCTs) reporting data on pharmacist-led discharge counseling.
DATA EXTRACTION: Primary extracted outcomes were emergency department visits and hospital readmission rates.
DATA SYNTHESIS: Meta-analyses of intervention versus usual care for hospital readmission and emergency department visit rates were performed using the inverse variance method. Results are reported as risk ratios (RRs) with 95% confidence intervals (CIs). Prediction intervals (PIs) were also calculated. Sensitivity and subgroup analyses were performed. A total of 21 RCTs were included in the qualitative synthesis and 18 in the meta-analyses (n = 7,244 patients). The original meta-analysis revealed a significant difference in the impact between pharmacist-led discharge counseling and usual care on overall hospital readmission (RR = 0.864 [95% CI 0.763-0.997], P = .020) and emergency department (RR = 0.697 [95% CI 0.535-0.907], P = .007) visits. However, the small number of included studies, the high heterogeneity among trials (I2 between 40% and 60%), and the wide PIs (hospital readmission: PI 0.542-1.186; emergency department visits: PI 0.027-1.367) prevented drawing further conclusions.
CONCLUSIONS: Insufficient evidence exists regarding the effect of pharmacist-led discharge counseling on hospital readmission and emergency department visits. Further well-designed clinical trials with defined core outcome sets are needed.
© 2020 Society of Hospital Medicine
The baseline characteristics of the included studies are presented in the Table. A total of 7,244 patients were included in this systematic review, most of them being 60 years or older (81%) and presenting chronic conditions (38.1%) such as cardiovascular and respiratory diseases. The majority of studies were performed in Europe (42.85%), followed by those conducted in the United States of America (28.6%). Overall, studies were classified as high risk of bias (57.14%), because most of them presented two or more domains with unclear risk of bias, especially due to the attrition domain (see Supplemental Material for complete analyses). Given the complexity of pharmacist interventions and the impossibility of blinding participants and personnel, the performance domain of the risk of bias tool was not assessed. Only three studies were considered as low risk of bias for all domains.22,37,40 Analyses on publication bias were performed by visualization of funnel plots and showed overall symmetry in all cases, which demonstrates a relative lack of bias. Few studies contributed to a slight asymmetry in the plots. Additional information is found in the Supplemental Material.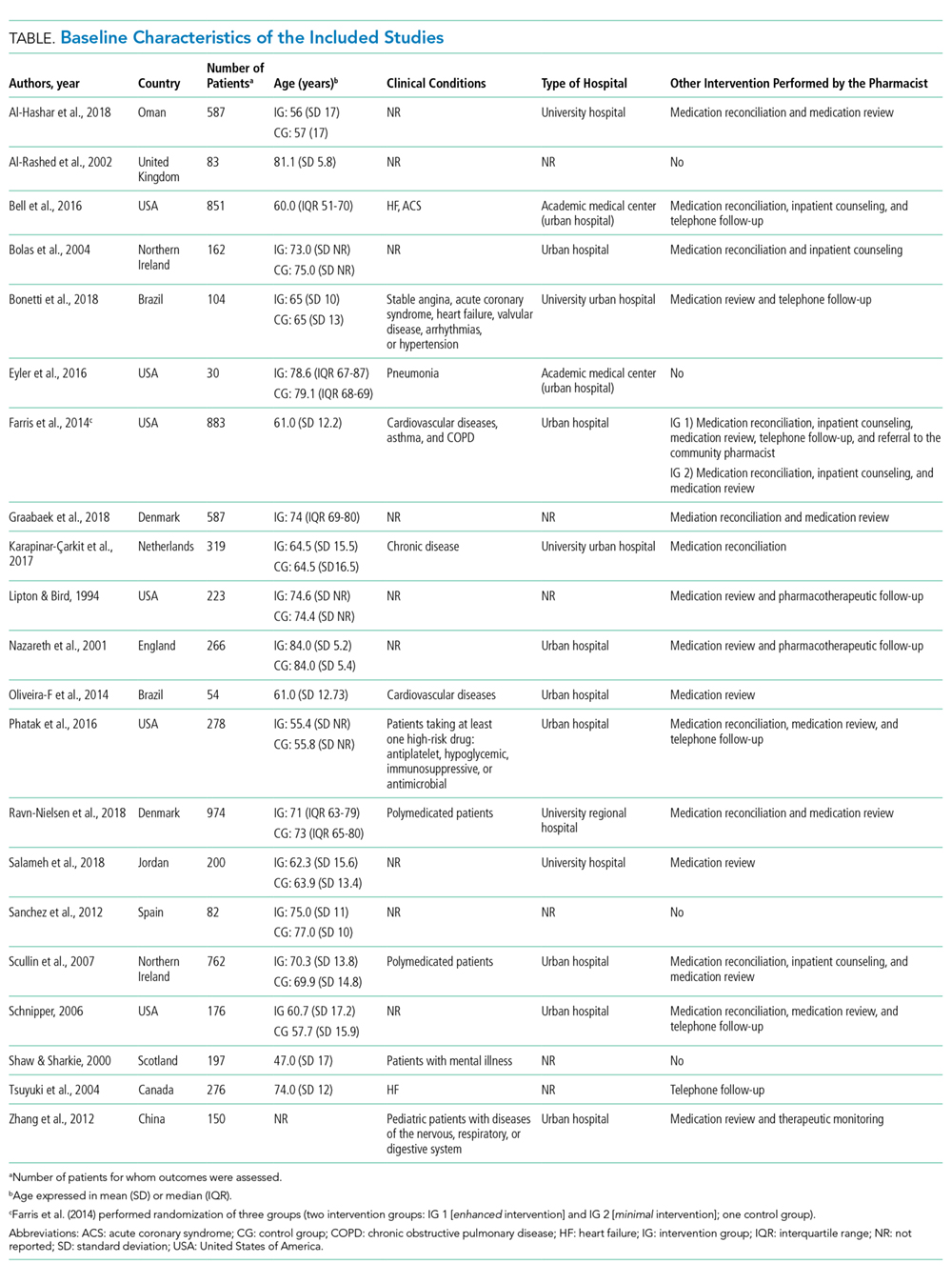
The detailed results for the pharmacist-led discharge medication counseling in each of the 21 included studies are presented in the Supplemental Material. The period of evaluation of the outcomes varied from two weeks (two studies) to one year after discharge (two studies). Only five studies showed statistically significant reductions in the number of hospital readmissions or emergency department visits in the group receiving pharmacist-led discharge counseling.21,24,32,35,36
Readmission Rates
A total of 18 studies evaluating the impact of pharmacist-led discharge counseling on hospital readmission were included in the meta-analysis.21,22,24-36,38-40 The studies by Al-Hashar et al., Bolas et al., and Schnniper et al. were excluded from statistical analyses due to a lack of sufficient data.20,23,27 The results revealed statistical differences between the intervention and usual care (RR = 0.864 [95% CI 0.763-0.997], P = .020; Figure 2). However, the heterogeneity among studies was high (I2 approximately 50%) and the calculation of PI revealed a wider interval, with the loss of the statistical significance (Tau = 0.151; PI 0.542-1.186). Sensitivity analyses with the hypothetical removal of trials showed few reductions in heterogeneity (I2 values ranging from 35.37% to 49.53%) with similar effect size values.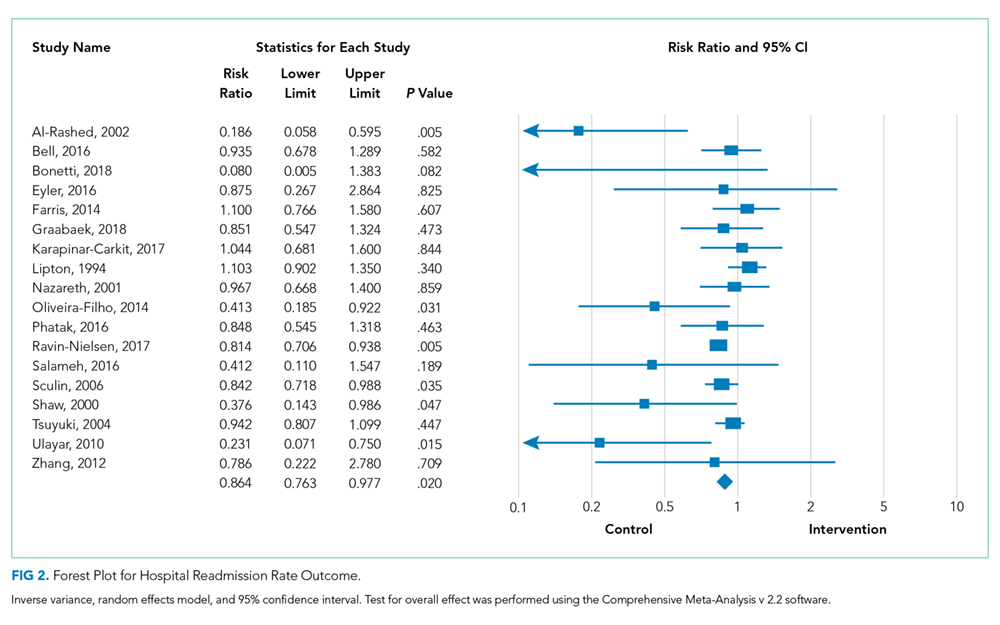
Subgroup analyses considering the time of hospital admission postdischarge (groups for two to three weeks, one month, three months, six months, and one year) did not demonstrate that pharmacist-led counseling reduced the number of hospital readmissions at any time (see Supplemental Material). Again, more than one study contributed to the moderately high heterogeneity in some subgroups (initial I2 values of 49.69% [one month], 69.43% [three months], 50.99% [six months], and 65.55% [one year]). The subgroups of two to three weeks and six months included few studies and caution should be used when interpreting such results (small meta-analysis with wide CIs; I2 value of 0%). Sensitivity analyses did not modify the original results (I2 values ranging from 35.37% to 49.56%).
In the subgroup analyses of how pharmacist interventions were delivered (ie, discharge counseling alone or combined with other interventions), interventions were superior to usual care, but again, few studies were evaluated, and the sensitivity analyses and calculation of PI revealed no true differences between groups. The meta-analysis for discharge counseling alone presented an RR of 0.333 (95% CI 0.129-0.858, P = .023; Supplemental Material), with three studies included (I2 = 48.0%, and Tau = 0.582, PI –11.221-11.880).21,25,35 The meta-analysis of other interventions showed an RR of 0.898 (95% CI 0.813-0.991, P = .033) (I2 = 28.9%; PI 0.690-1.099).22,24-36,38-40 The detailed results of PIs are reported in the Supplemental Material.
