Aspiration Pneumonia in Older Adults





Aspiration pneumonia refers to an infection of the lung parenchyma in an individual that has inhaled a bolus of endogenous flora that overwhelms the natural defenses of the respiratory system. While there are not universally agreed upon criteria, the diagnosis can be made in patients with the appropriate risk factors and clinical scenario, in addition to a radiographic or an ultrasonographic image of pneumonia in the typical dependent lung segment. Treatment options for aspiration pneumonia vary based on the site of acquisition (community-acquired aspiration pneumonia [CAAP] versus healthcare-associated aspiration pneumonia [HCAAP]), the risk for multidrug-resistant (MDR) organisms, and severity of illness. Hospitalized CAAP patients without severe illness and with no risk for MDR organisms or Pseudomonas aeruginosa (PA) can be treated with standard inpatient community-acquired pneumonia therapy covering anaerobes. Patients with CAAP and either of the following—risk factors for MDR pathogens, septic shock, need for an intensive care unit (ICU) admission, or mechanical ventilation—can be considered for broader coverage against anaerobes, methicillin-resistant Staphylococcus aureus (MRSA), and PA. Severe aspiration pneumonia that originates in a long-term care facility or HCAAP with one or more risk factors for MDR organisms should be considered for similar treatment. HCAAP with one or more risk factors for MDR organisms or PA, plus septic shock, need for ICU admission or mechanical ventilation should receive double coverage for PA in addition to coverage for MRSA and anaerobes. Multiple gaps in current understanding and management of aspiration pneumonia require future research, with a particular focus on antibiotic stewardship.
© 2019 Society of Hospital Medicine
Risk Factors for Aspiration Pneumonia
Risk factors for aspiration pneumonia, while not universally agreed upon, are important to recognize as they increase the probability of the diagnosis when present. A 2011 systematic review identified age, male gender, lung disease, dysphagia, and diabetes mellitus (level 2a), as well as severe dementia, angiotensin I-converting enzyme deletion/deletion genotype, and poor oral health (level 2b) as risk factors.13 In 2016, a panel of experts reached a consensus (modified Delphi Method) on the following risk factors for the diagnosis of aspiration pneumonia in nursing home residents: history of dysphagia, choking incident, tube feeding, neurologic disease, and cognitive impairment. The presence of one or more of these risk factors in the appropriate clinical setting may suggest a diagnosis of aspiration pneumonia.14
Radiographic/Ultrasonographic Imaging
In the appropriate scenario, the diagnosis of aspiration pneumonia is supported with an image representative of pneumonia. The pulmonary segment involved in aspiration pneumonia depends on the position of the patient during the aspiration event. If the aspiration event occurs while the patient is in the recumbent position, development of pneumonia is more common in the posterior segments of the upper lobes and the apical segments of the lower lobes; whereas if it occurs while the patient is in an upright position, the location changes to the basal segments of the lower lobes.3
Overall, the sensitivity of a chest X-ray to diagnose pneumonia ranges between 32%-77.7%,15-17 suggesting that a significant proportion of patients suspected of having pneumonia in past research studies, may have been misdiagnosed. Studies using lung ultrasound to identify pneumonia demonstrate a higher sensitivity, but additional research is needed to validate these findings.17-19 Noncontrast CT scans of the chest remain the reference standard for diagnosing pneumonia and currently tend to have the largest impact on diagnosis and subsequent treatment decisions.15,16,20,21 As a result, if radiation exposure risks are not a concern for the patient, we recommend utilizing noncontrast CT imaging whenever the diagnosis is in doubt until future research elucidates the most appropriate approach to imaging.
Diagnosis
Diagnosing aspiration pneumonia is difficult, in part because there is no universal definition or set of diagnostic criteria. The diagnosis of aspiration pneumonia is supported by the fulfillment of three criteria. First, appropriate risk factors for aspiration, as documented above, should be present. Second, there should be evidence of clinical signs and symptoms of pneumonia (typical or atypical). Third, radiographic representation of pneumonia in a dependent pulmonary segment confirms the diagnosis. Once these criteria are met, it is important to distinguish between CAAP and HCAAP with particular attention to risk factors for multidrug-resistant (MDR) organisms and Pseudomonas aeruginosa (PA).
MICROBIOLOGY
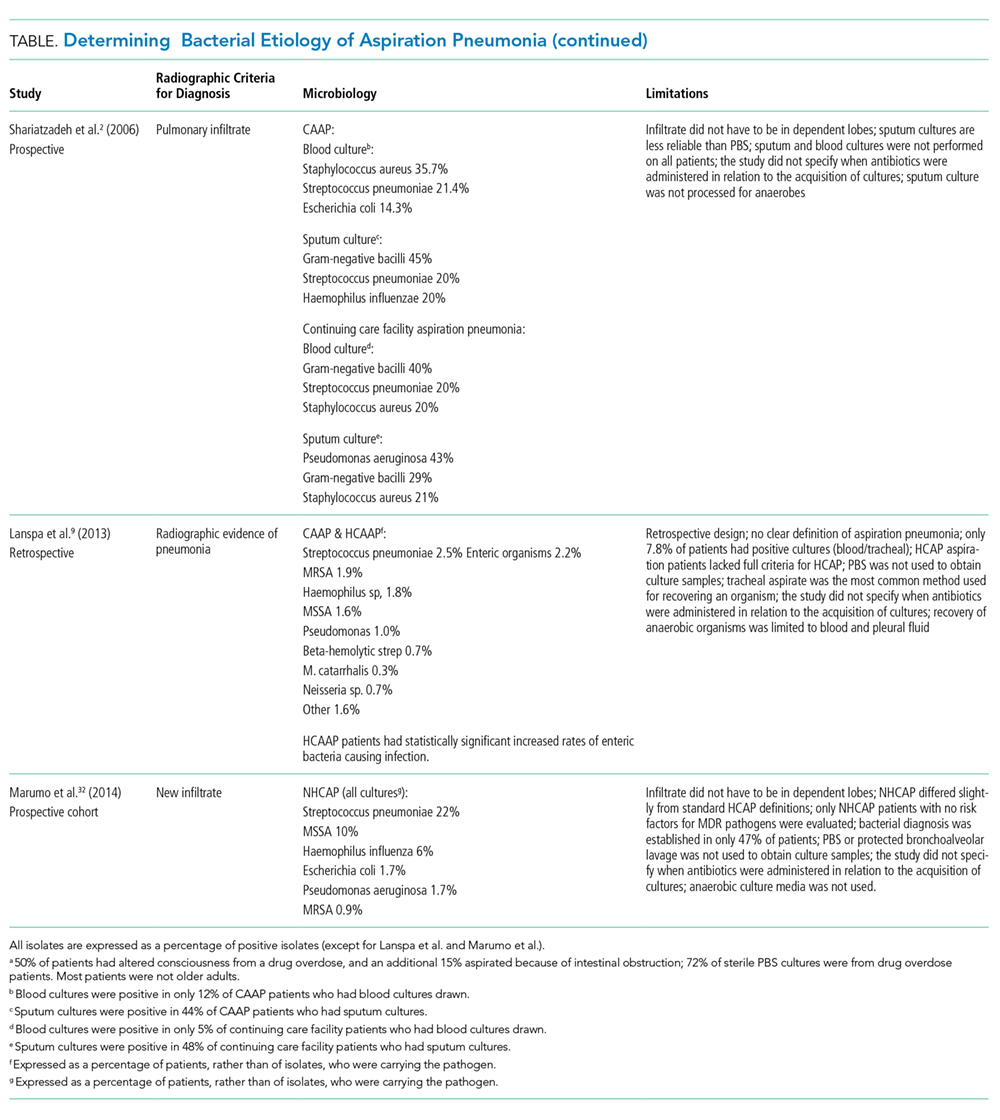
Many studies have tried to determine the exact bacterial etiology of aspiration pneumonia as documented in the Table.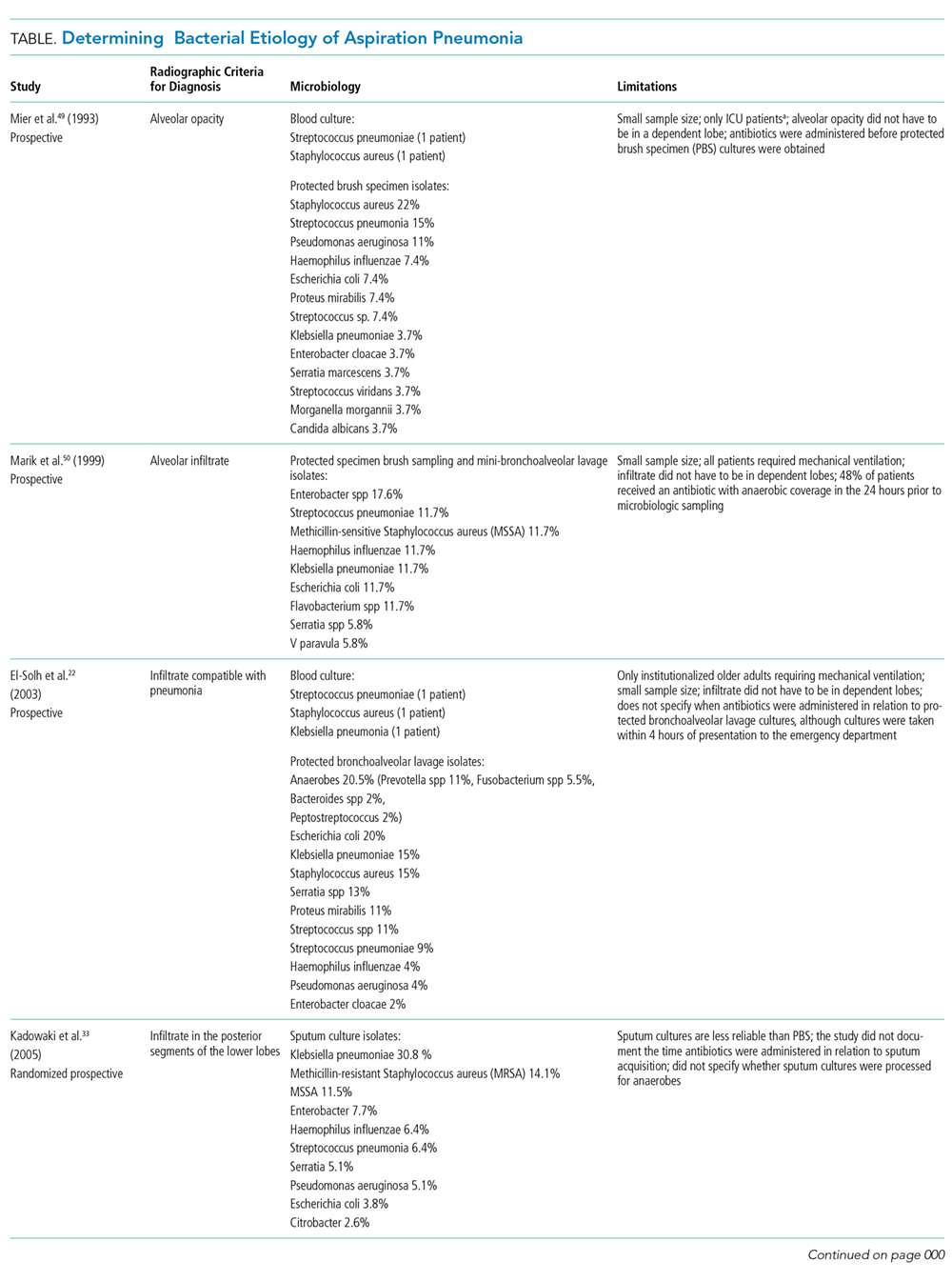
Even when an ideal method is used to obtain a good sample, however, the results are limited by other variables in the study. For example, in studies that use protected brush specimens and protected bronchoalveolar lavage to acquire samples for culture, many patients received antibiotics prior to sampling, and the studies are small (Table). Although anaerobes have traditionally been implicated in aspiration pneumonia, only El-Solh et al.22 were able to culture a significant proportion of anaerobes. The study, however, was limited to institutionalized older adults requiring mechanical ventilation and it did not require the typical radiographic location for aspiration pneumonia. Even under the best circumstances, it is difficult to determine causality because the antibiotics used to treat these cases of aspiration pneumonia cover a broad range of organisms. Based on the studies in the Table, causative organisms may include Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, and gram-negative rods in addition to traditional organisms classically thought to cause aspiration pneumonia-anaerobes. Microbiologic etiology, however, may also be insinuated from the studies discussed in the therapeutic strategies section below as some include antibiotics with limited antimicrobial activity.