Serious Choices: A Systematic Environmental Scan of Decision Aids and Their Use for Seriously Ill People Near Death





Seriously ill people near death face difficult decisions about life-sustaining treatments such as cardiopulmonary resuscitation and mechanical ventilation. Patient decision aids may improve alignment between patients’ preferences and the care they receive, but the quantity, quality, and routine use of these tools are unknown. We conducted a systematic environmental scan to identify all decision aids for seriously ill people at high risk of death facing choices about life-sustaining treatments, assess their quality, and explore their use in clinical settings. We searched MEDLINE, Google, and mobile application stores and surveyed experts. We included 27 decision aids in our scan. Concerning content, 14 of 27 decision aids for seriously ill people near death were for people with specific diseases and conditions (ie, advanced cancer or kidney disease); 11 concerned individual life-sustaining treatment decisions (ie, cardiopulmonary resuscitation or mechanical ventilation). Only two focused on more general care pathways (ie, life-sustaining intervention, palliative care, and hospice). Twenty-four of 27 decision aids presented options in a balanced way; 23 identified funding sources, and 19 of 27 reported their publication date. Just 11 used plain language. A minority, 11 of 27, listed evidence sources, five documented rigorous evidence-synthesis methods, six disclosed competing interests, and three offered update policies. Preliminary results suggest that few health systems use decision aids in routine patient care. Although many decision aids exist for life-sustaining treatment decisions during serious illness, the tools are deficient in some key quality areas.
© 2019 Society of Hospital Medicine
Decision Aid Search Strategy
We searched for patient decision aids among published systematic reviews, Internet search results (Google.com), and app stores (Google Play and Apple App Store). To identify previously published systematic reviews, we searched MEDLINE via PubMed, with the date range from inception to 2017. We chose not to include other academic databases because the unit of observation for this environmental scan was the decision aids themselves, not the published articles. Additionally, we were aware of systematic reviews concerning this issue and felt that adding additional databases would not appreciably improve our likelihood of identifying eligible decision aids. We conducted searches using Google.com on November 30, 2016, and January 26, 2017, and included the first 100 search results. We also contacted shared decision-making and palliative care experts using a previously established list, via an online survey and one-on-one interviews between April 17, 2017, and August 30, 2017.
Published Reviews
Using a search strategy developed with a librarian, we identified reviews of decision aids that met our inclusion criteria using the MEDLINE database.17 The primary reviewer (CHS) examined the results of the search, identifying reviews appropriate for further investigation and the secondary reviewer (KP) extracted patient decision aids potentially eligible for our study. See Appendix Table 1 and our published protocol.17 Notably, given that the decision aids themselves, not published articles, were the unit of observation for our environmental scan, we did not perform dual coding on the MEDLINE extraction.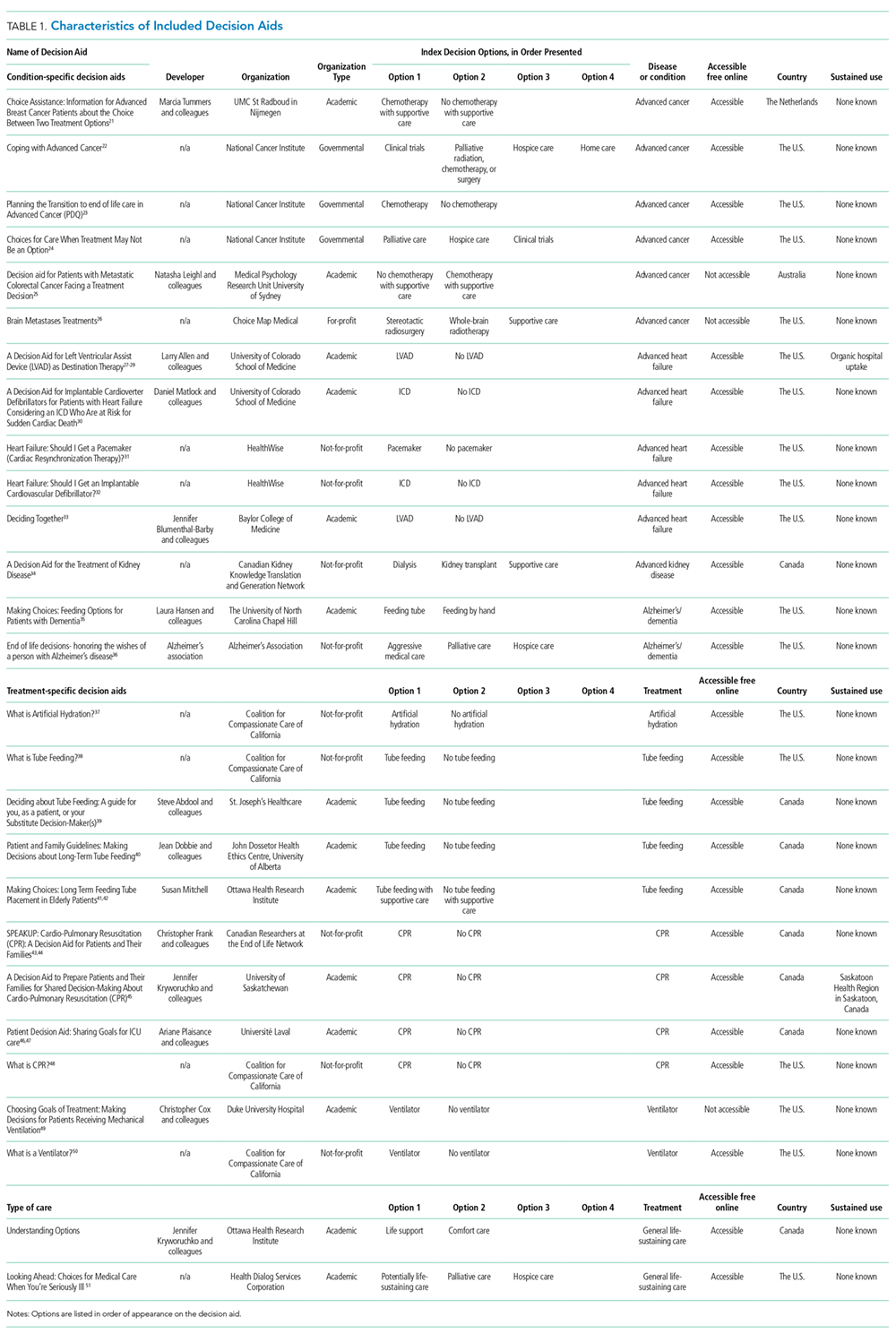
Google and App Stores
Two reviewers (CHS and MAD) performed the Google and application screening, including both the Apple App Store and Google Play.17 Using Google Advanced Search, we ran the queries detailed in Appendix Table 2. We disabled cookies and limited our search to English.
The primary reviewer ran each Google search and app store search, archiving the first 100 results of Google searches and first 50 results of app store searches.18 Then, the primary reviewer opened each page and scanned for patient decision aids or references to patient decision aids, marking those that met our inclusion criteria, those that might meet our inclusion criteria with further research, and those that were not appropriate. We documented specific reasons for exclusion. The secondary reviewer assessed a randomly-selected, 10% subsample. We calculated interrater reliability using a Cohen’s Kappa statistic.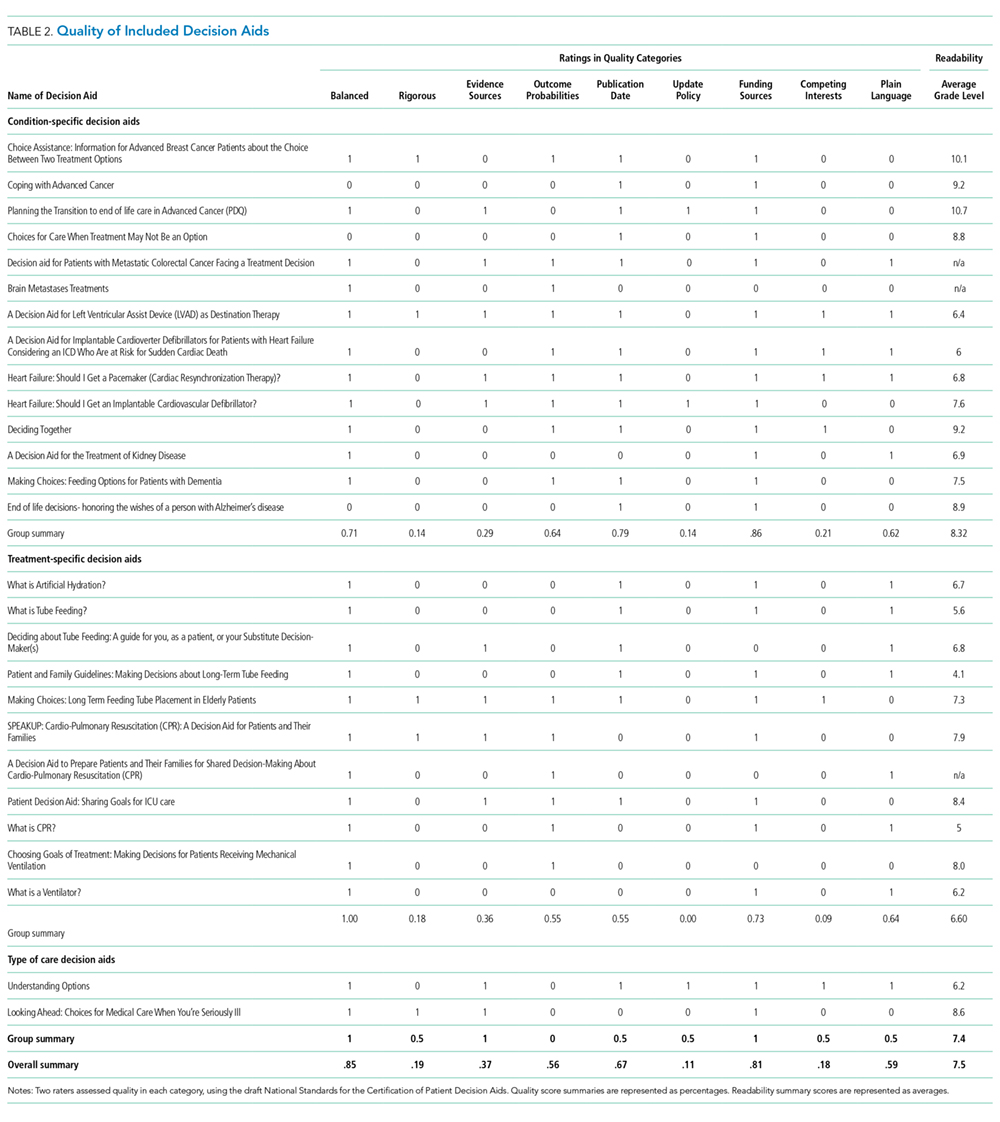
Key Informants
To identify decision aids that did not appear in our online search, we surveyed 187 key informants who work in or study issues related to aging, death and dying and shared decision making.19 We developed a questionnaire for these informants and deployed it using the online survey software Qualtrics (see Appendix 1. Key Informant Survey). We used a snowball approach, asking participants for other individuals they thought we should speak with about other relevant decision aids. We corresponded with individuals who suggested decision aids that were not already in our decision aid database.
Decision Aid Selection Criteria
We included patient decision aids designed to help seriously ill people near death or their caregivers make decisions about life-sustaining treatments. See Appendix Table 1 for an explanation of terms. We saved decision aids that met our inclusion criteria in an online database, organizing them by target user or index decision(s). When identified decision aids were unavailable online, we e-mailed developers three times to ask for access to the decision aid. If after three queries, we did not receive access to the decision aid, we excluded the tool from our review. Similarly, if developers explicitly refused to participate in the study, we excluded them.
