Prospective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI)





BACKGROUND: Intraoperative hypotension is associated with an increased risk of end organ damage and death. The transient preoperative interruption of angiotensin-converting enzyme inhibitor (ACEI) therapy prior to cardiac and vascular surgeries decreases the occurrence of intraoperative hypotension.
OBJECTIVE: We sought to compare the effect of two protocols for preoperative ACEI management on the risk of intraoperative hypotension among patients undergoing noncardiac, nonvascular surgeries.
DESIGN: Prospective, randomized study.
SETTING: Midwestern urban 489-bed academic medical center.
PATIENTS: Patients taking an ACEI for at least six weeks preoperatively were considered for inclusion.
INTERVENTIONS: Randomization of the final preoperative ACEI dose to omission (n = 137) or continuation (n = 138).
MEASUREMENTS: The primary outcome was intraoperative hypotension, which was defined as any systolic blood pressure (SBP) < 80 mm Hg. Postoperative hypotensive (SBP < 90 mm Hg) and hypertensive (SBP > 180 mm Hg) episodes were also recorded. Outcomes were compared using Fisher’s exact test.
RESULTS: Intraoperative hypotension occurred less frequently in the omission group (76 of 137 [55%]) than in the continuation group (95 of 138 [69%]) (RR: 0.81, 95% CI: 0.67 to 0.97, P = .03, NNH 7.5). Postoperative hypotensive events were also less frequent in the ACEI omission group (RR: 0.49, 95% CI: 0.28 to 0.86, P = .02) than in the continuation group. However, postoperative hypertensive events were more frequent in the omission group than in the continuation group (RR: 1.95, 95%: CI: 1.14 to 3.34, P = .01).
CONCLUSION: The transient preoperative interruption of ACEI therapy is associated with a decreased risk of intraoperative hypotension.
REGISTRATION: ClinicalTrials.gov: NCT01669434.
© 2018 Society of Hospital Medicine
We estimated that a sample size of 300 patients would achieve 80% power to detect a difference of 0.17 between the group proportions of 0.33 and 0.50 at a significance level (ɑ) of 0.05 by using a two-sided z-test with continuity correction, assuming 15% loss to follow-up. This estimate allowed for 1 interim analysis using the O’Brien-Fleming spending function truncated at three standard deviations to determine the test boundaries. The monitoring boundary P values associated with the interim analysis were .003, and the threshold P value for the final analysis was .049.
RESULTS
Study Flow
A total of 453 patients were screened for eligibility. Among these patients, 162 were excluded, and the remaining 291 patients were randomized (Figure 1). Surgery was cancelled in six patients allocated to omission and in four patients allocated to continuation arms, respectively. Moreover, three patients in the omission arm were excluded from the analysis following randomization. Specifically, one was excluded because of early discharge without overnight stay, one was excluded because of withdrawal of consent, and one was excluded because of missing primary outcome data. In addition, three cases in the continuation arm were excluded following randomization because of the preoperative (permanent) discontinuation of ACEI therapy in two cases and discharge without an overnight stay in one case. Finally, 275 patients were included in the analysis: 137 in the ACEI omission group and 138 in the ACEI continuation group. Adherence to allocation was 88% and 92% in the omission and continuation groups, respectively.
Baseline Characteristics
The demographic data of patients allocated to ACEI omission and those allocated to ACEI continuation were similar (Table 1). A large majority of patients in both groups took the ACEI lisinopril. Overall, 187 of 275 (68%) patients were taking at least 1 antihypertensive agent, most commonly a diuretic, in addition to an ACEI. SBP measured during the preoperative clinic visit averaged 136.5 mm Hg and did not differ significantly between groups (P = .84).
Surgical Variables
General anesthesia was the most commonly utilized technique, although spinal and regional anesthesia were also represented (Table 1). The majority of cases in both groups were planning for orthopedic and spinal surgery. The method of anesthesia or type of surgery between patients allocated to ACEI omission and those allocated to continuation did not differ (P = .61 and P = .45 respectively).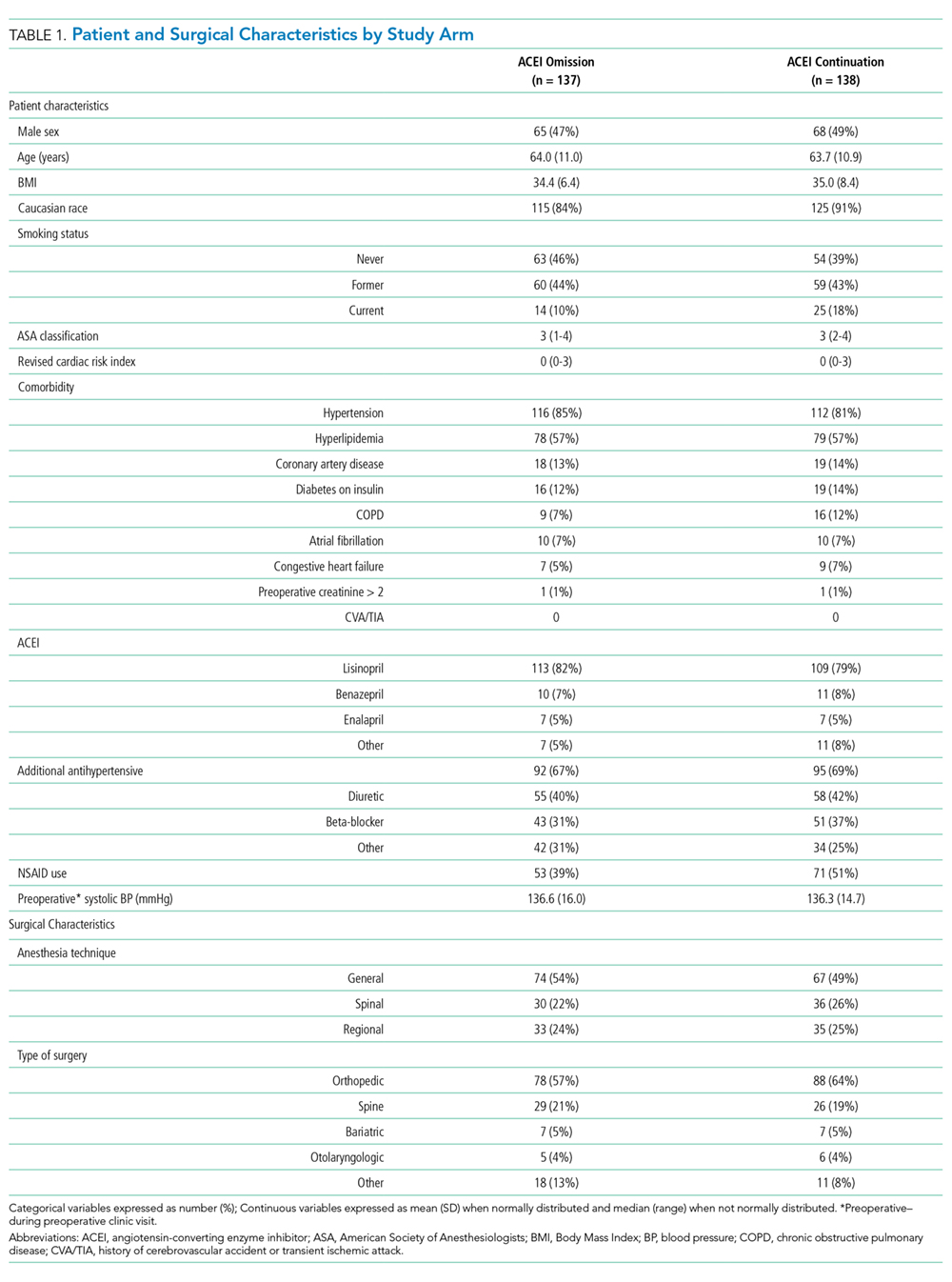
Episodes of Intraoperative Hypotension
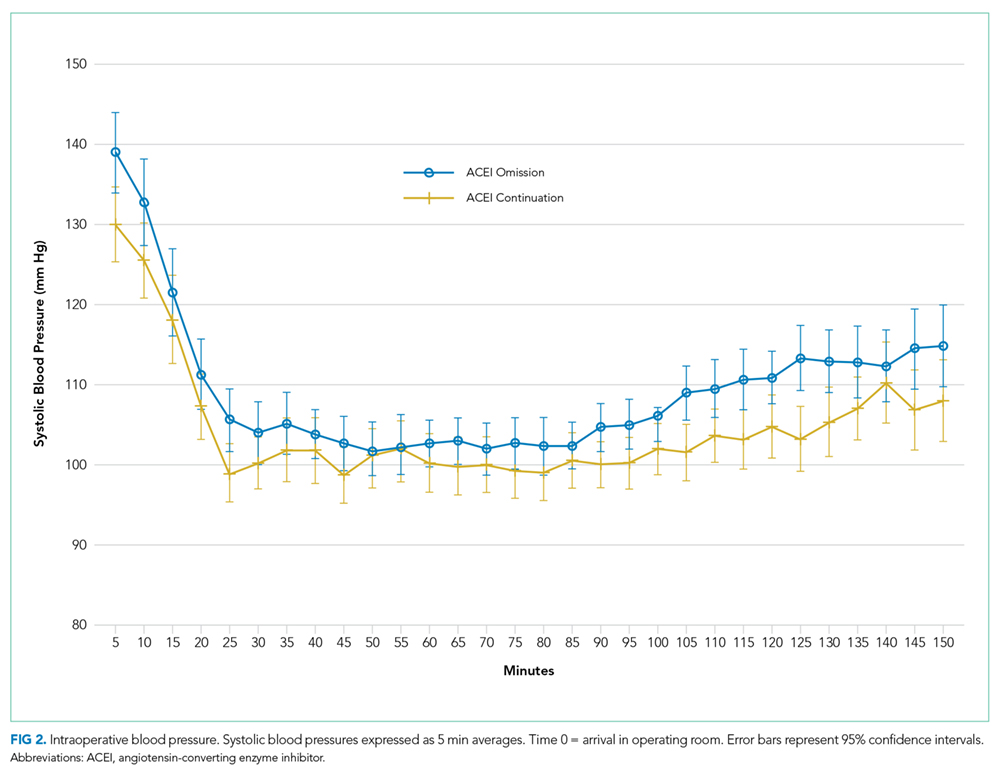
Intraoperative SBPs are displayed in Figure 2, and hemodynamic outcomes are summarized in Table 2. Episodes of SBP < 80 mm Hg during anesthesia induction were numerically less frequent in the omission group than in the continuation group; the difference between groups, however, was not statistically significant (24 of 137 [18%] vs 38 of 138 [28%], RR: 0.64, 95% CI: 0.40 to 1.00, P = .06).