Hospital Readmissions in Patients with Cirrhosis: A Systematic Review





BACKGROUND: Hospital readmission is a significant problem for patients with complex chronic illnesses such as liver cirrhosis.
PURPOSE: We aimed to describe the range of readmission risk in patients with cirrhosis and the impact of the model for end-stage liver disease (MELD) score.
DATA SOURCES: We conducted a systematic review of studies identified in Ovid MEDLINE, PubMed, EMBASE, CINAHL, the Cochrane Library, Scopus, Google Scholar, and ClinicalTrials.gov from 2000 to May 2017.
STUDY SELECTION: We examined studies that reported early readmissions (up to 90 days) in patients with cirrhosis. Studies were excluded if they did not examine the association between readmission and at least 1 variable or intervention.
DATA EXTRACTION: Two reviewers independently extracted data on study design, setting, population, interventions, comparisons, and detailed information on readmissions.
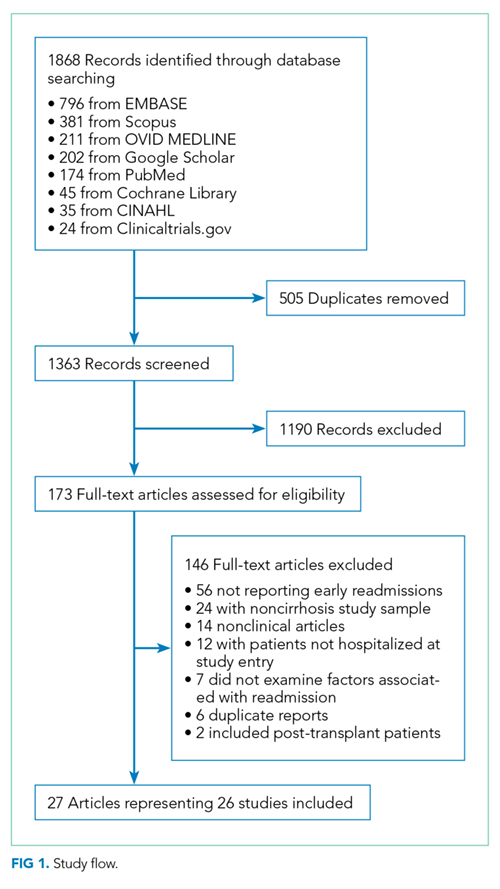
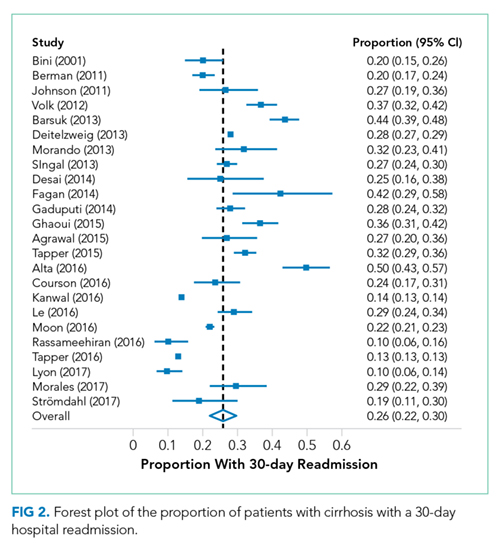
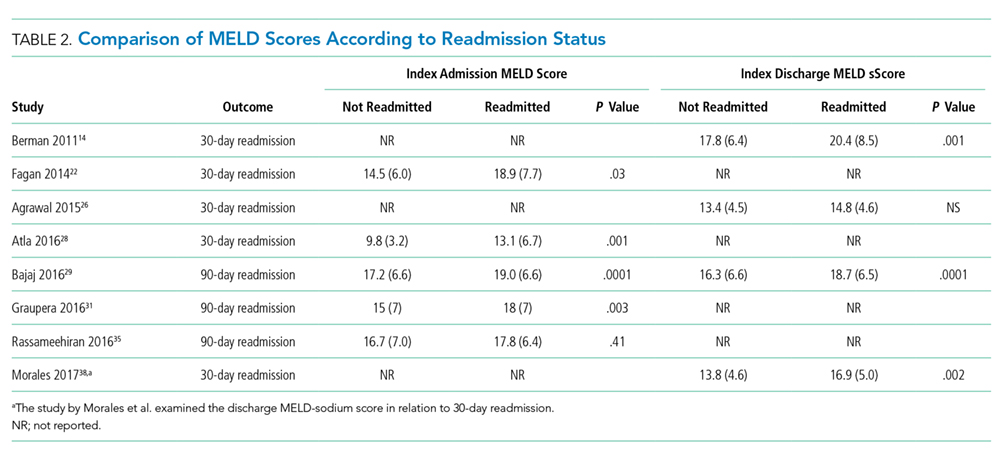
DATA SYNTHESIS: Of the 1363 records reviewed, 26 studies met the inclusion and exclusion criteria. Of these studies, 21 were retrospective, and there was significant variation in the inclusion and exclusion criteria. The pooled estimate of 30-day readmissions was 26%(95% confidence interval [CI], 22%-30%). Few studies examined readmission preventability or the relationship between readmissions and social determinants of health. Reasons for readmission were highly variable. An increased MELD score was associated with readmissions in most studies. Readmission was associated with increased mortality.
CONCLUSION: Hospital readmissions frequently occur in patients with cirrhosis and are associated with liver disease severity. The impact of functional and social factors on readmissions is unclear.
© 2018 Society of Hospital Medicine
Statistical Analysis
Analyses were performed using Stata 13.1 (StataCorp LP, College Station, Texas). We determined the pooled proportion of patients with 30-day readmission using a random-effects model, with the Freeman–Tukey double-arcsine transformation for meta-analysis of proportions.12 We investigated the heterogeneity by stratifying analyses according to prespecified study characteristics, including “broad” versus “focused.” However, the readmission risk was not different in the stratified analysis; therefore, we chose to pool the findings. For point estimates, 95% confidence intervals (CIs) were calculated, and a P-value < .05 was considered statistically significant.
RESULTS
Search Results
Study Characteristics
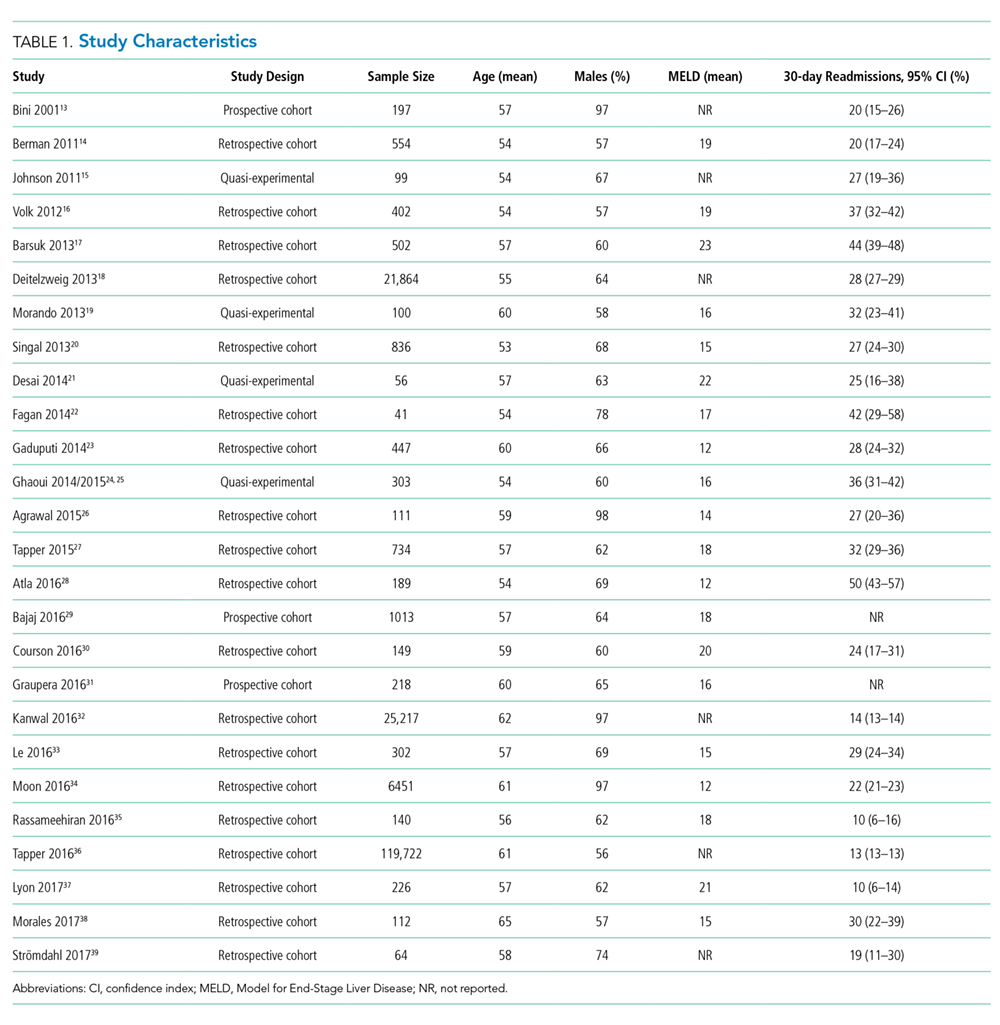
Two studies were performed in Australia, 4 in Europe, and the remainder in North America. Twenty one of the 26 studies were retrospective cohort studies (Table 1). Twenty studies were single-center studies (of which half were performed at transplant centers), and 4 of the 6 multicenter studies were based on administrative data with large samples (173,254 patients). The inclusion/exclusion criteria varied widely (Supplementary Material). Some studies only included patients admitted for specific cirrhosis complications, while others included those admitted for any reason. Two studies excluded patients admitted in the prior 30 days, and 6 excluded patients discharged to hospice. The mean risk of bias score was 7.5 (SD 1.3) out of a possible 9 points, with most lacking an adequate description of follow-up and several lacking adjustment for confounders.
Outcomes
Readmission and MELD
DISCUSSION
Hospital readmission is a costly and common problem in the US.2 In addition to the negative impact that readmissions have on patients’ lives,40 readmissions are increasingly being used to measure quality. Unplanned 30-day readmissions are posted publicly, and excess readmissions for high-risk conditions are penalized through HRRP.3 Although HRRP does not currently include cirrhosis, the program has expanded to include several conditions that were not included in the initial iteration. Whether cirrhosis will be included in future iterations remains to be seen; however, increasing scrutiny is likely to continue. Of specific populations at risk, patients with cirrhosis are particularly vulnerable due to several features. Ascites management often requires hospitalization due to diuretic titration and poor access to paracentesis, and hepatic encephalopathy treatment requires complex lactulose titration.16 Other features of cirrhosis, such as gastrointestinal bleeding, infections, and renal failure, also place patients at risk of poor outcomes. The resulting readmission burden is high, with a pooled 30-day readmission rate of 26%. Other associated outcomes are also poor, with a consistent relationship between readmission and subsequent mortality.
