Safe Opioid Prescribing for Acute Noncancer Pain in Hospitalized Adults: A Systematic Review of Existing Guidelines





BACKGROUND: Pain is common among hospitalized patients. Inpatient prescribing of opioids is not without risk. Acute pain management guidelines could inform safe prescribing of opioids in the hospital and limit associated unintended consequences.
PURPOSE: To evaluate the quality and content of existing guidelines for acute, noncancer pain management.
DATA SOURCES: The National Guideline Clearinghouse, MEDLINE via PubMed, websites of relevant specialty societies and other organizations, and selected international search engines.
STUDY SELECTION: Guidelines published between January 2010 and August 2017 addressing acute, noncancer pain management among adults were considered. Guidelines that focused on chronic pain, specific diseases, and the nonhospital setting were excluded.
DATA EXTRACTION: Quality was assessed using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument.
DATA SYNTHESIS: Four guidelines met the selection criteria. Most recommendations were based on expert consensus. The guidelines recommended restricting opioids to severe pain or pain that has not responded to nonopioid therapy, using the lowest effective dose of short-acting opioids for the shortest duration possible, and co-prescribing opioids with nonopioid analgesics. The guidelines generally recommended checking the prescription drug monitoring program when prescribing opioids, developing goals for patient recovery, and educating patients regarding the risks and side effects of opioid therapy. Additional recommendations included using an opioid-dose conversion guide, avoidance of co-administration of parenteral and oral opioids, and using caution when co-prescribing opioids with other central nervous system depressants.
CONCLUSIONS: Guidelines, based largely on expert opinion, recommend judicious prescribing of opioids for severe, acute pain. Future work should assess the implications of these recommendations on hospital-based pain management.
© 2018 Society of Hospital Medicine
Guideline Quality Assessment
Guideline Synthesis and Analysis
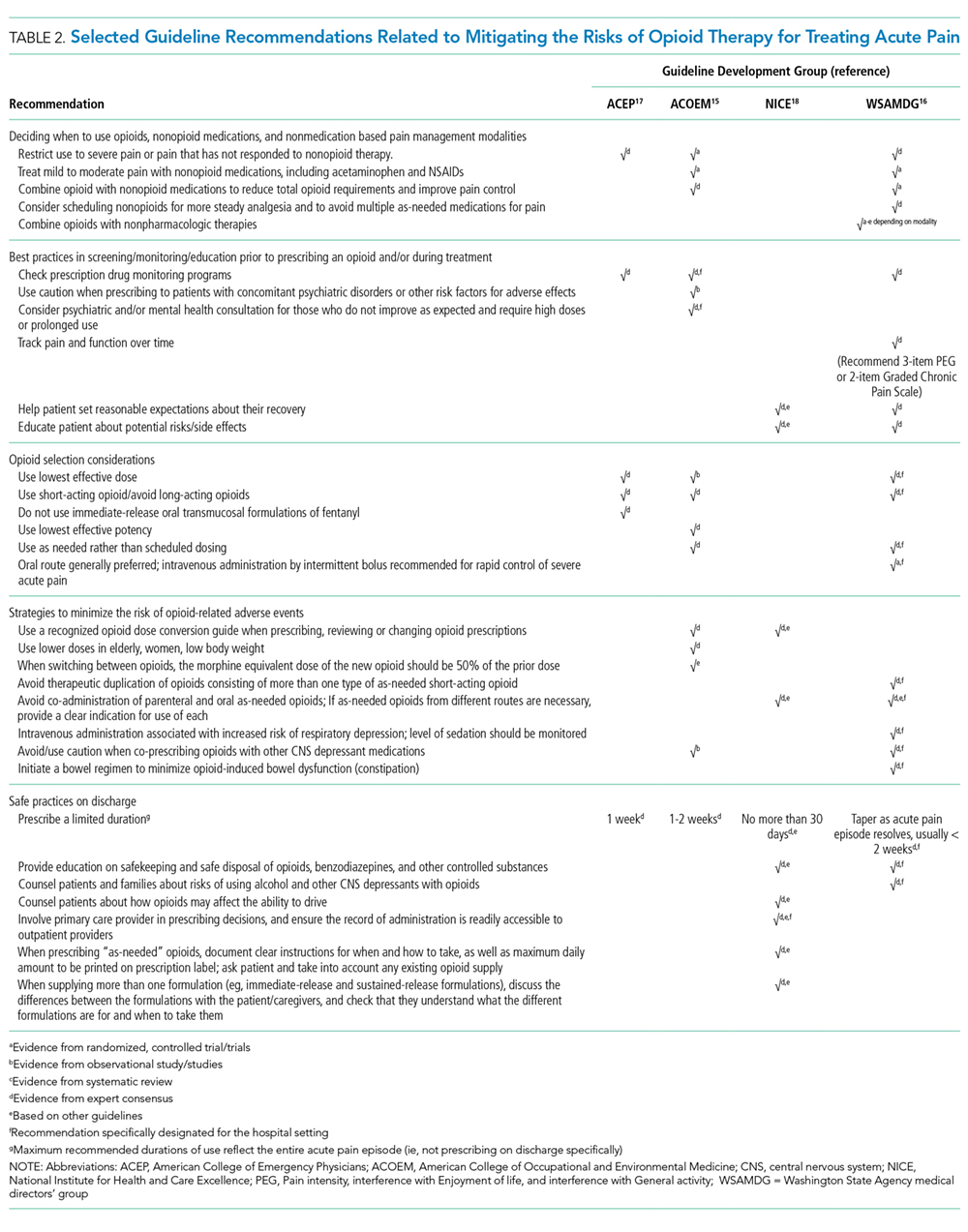
We extracted recommendations from each guideline related to the following topics: 1) deciding when to use opioids, nonopioid medications, and nonmedication-based pain management modalities, 2) best practices in screening/monitoring/education prior to prescribing an opioid and/or during treatment, 3) opioid selection considerations, including selection of dose, duration, and route of administration, 4) strategies to minimize the risk of opioid-related adverse events, and 5) safe practices on discharge.
Role of the Funding Source
The Society of Hospital Medicine provided administrative and material support for the project, but had no role in the design or execution of the scientific evaluation.
RESULTS
Guideline Quality Assessment
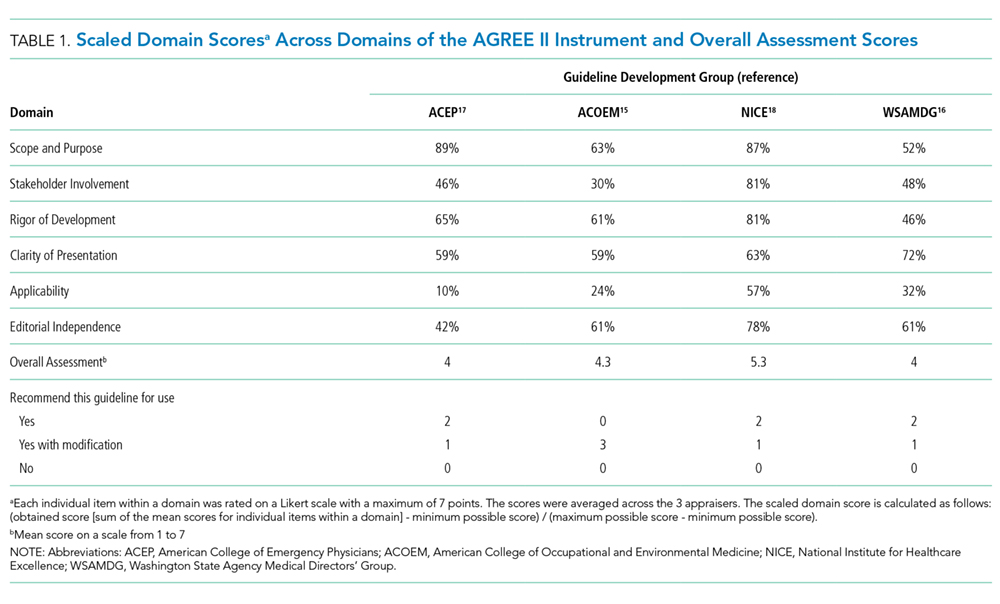
See Table 1 for the AGREE II scaled domain scores, and Appendix Table 1 for the ratings on each individual item within a domain. The range of scaled scores for each of the AGREE II domains were as follows: Scope and purpose 52%-89%, stakeholder involvement 30%-81%, rigor of development 46%-81%, clarity of presentation 59%-72%, applicability 10%-57%, and editorial independence 42%-78%. Overall guideline assessment scores ranged from 4 to 5.33 on a scale from 1 to 7. Three of the guidelines (NICE, ACOEM, and WSAMDG)16,17,19 were recommended for use without modification by 2 out of 3 guideline appraisers, and one of the guidelines (ACEP)18 was recommended for use with modification by all 3 appraisers. The guideline by NICE19 was rated the highest both overall (5.33), and on 4 of the 6 AGREE II domains.
Although the guidelines each included a systematic review of the literature, the NICE19 and WSAMDG17 guidelines did not include the strength of recommendations or provide clear links between each recommendation and the underlying evidence base. When citations were present, we reviewed them to determine the type of data upon which the recommendations were based and included this information in Table 2. The majority of the recommendations in Table 2 are based on expert opinion alone, or other guidelines.
Guideline Synthesis and Analysis
Table 2 contains a synthesis of the recommendations related to each of our 5 prespecified content areas. Despite the generally low quality of the evidence supporting the recommendations, there were many areas of concordance across guidelines.
Deciding When to Use Opioids, Nonopioid Medications, and Nonmedication-Based Pain Management Modalities
Three out of 4 guidelines recommended restricting opioid use to severe pain or pain that has not responded to nonopioid therapy,16-18 2 guidelines recommended treating mild to moderate pain with nonopioid medications, including acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs),16,17 and 2 guidelines recommended co-prescribing opioids with nonopioid analgesic medications to reduce total opioid requirements and improve pain control.16,17 Each of these recommendations was supported by at least one randomized controlled trial.
Best Practices in Screening/Monitoring/Education to Occur Prior to Prescribing an Opioid and/or During Treatment
Three guidelines recommended checking prescription drug monitoring programs (PDMPs), all based on expert consensus.16-18 Only the WSAMDG guideline offered guidance as to the optimal timing to check the PDMP in this setting, specifically recommending to check before prescribing opioids.17 Two guidelines also recommended helping patients set reasonable expectations about their recovery and educating patients about the risks/side effects of opioid therapy, all based on expert consensus or other guidelines.17,19
