A Single, Post-ACTH Cortisol Measurement to Screen for Adrenal Insufficiency in the Hospitalized Patient





BACKGROUND: Cosyntropin stimulation testing (CST) is used to screen patients for adrenal insufficiency (AI). Traditionally, CST includes baseline cortisol concentration, the administration of cosyntropin, and cortisol concentration at 30 and 60 minutes poststimulation. There is debate surrounding the utility of testing and cut-off points for concentrations at each time point.
OBJECTIVE: To determine if a single cortisol measurement at 30 or 60 minutes could replace the traditional approach.
DESIGN: We looked retrospectively at inpatients who underwent standard, high-dose CST (n = 702) and evaluated the number of patients who would screen positive for AI by using a single time point (30 or 60 minutes) compared with the traditional CST.
SETTING: A tertiary-care, academic medical center.
PATIENTS: Hospital inpatients present between January 2012 and September 2013.
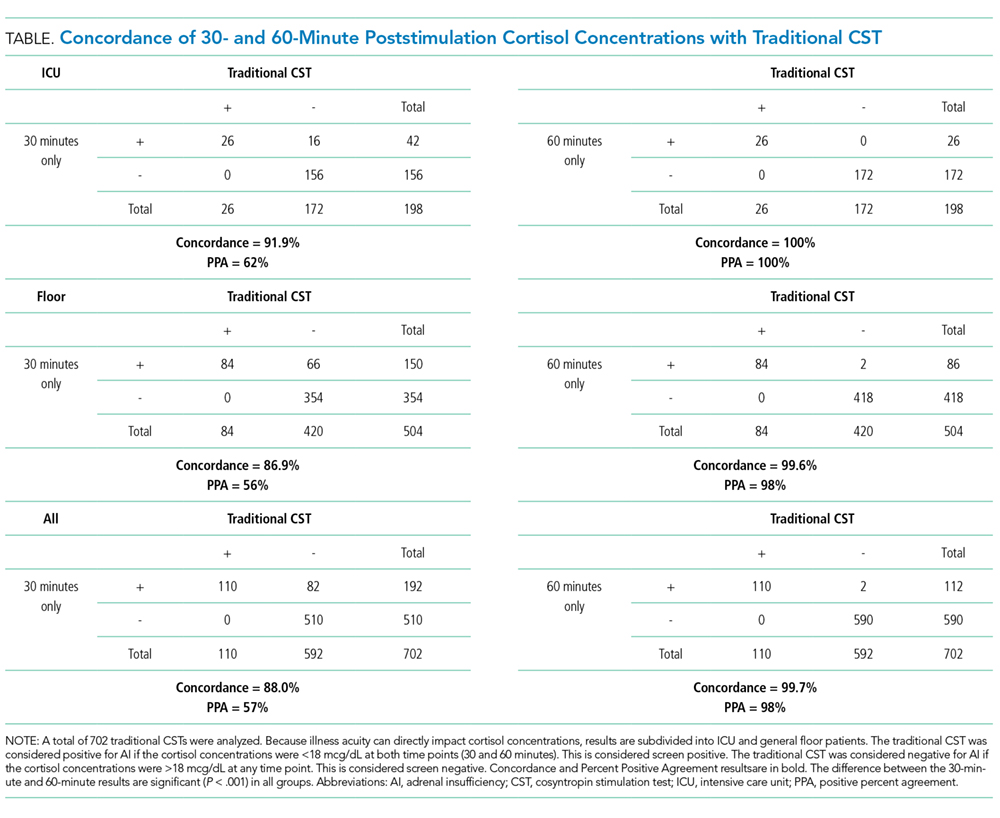
RESULTS: Of tests, 84.3% were normal, which was defined as at least 1 cortisol concentration of 18 mcg/dL or higher at any time after stimulation. The average 60-minute concentration was higher than the average 30-minute concentration (P < .001). A single 60-minute concentration is 100% concordant with the full CST in the intensive care unit (ICU) subgroup and 99.6% concordant in floor patients. A single 30-minute concentration is significantly less concordant, 91.9% and 86.9%, in the ICU and floor subgroups, respectively.
CONCLUSIONS: Overall, a single 60-minute cortisol concentration to screen for AI was 99.7% concordant with the traditional CST, and the positive percent agreement was 98%. Fewer false-positive screens would occur with a single 60-minute cortisol concentration compared with a single 30-minute concentration (P < .001). High-dose CST screening may safely be interpreted with single 60-minute poststimulation cortisol serum concentrations.
© 2018 Society of Hospital Medicine
Cortisol concentrations were assessed by the laboratory according to the manufacturer’s instructions by using the ADVIA Centaur Cortisol assay (Siemens Healthcare Diagnostics Inc, Tarrytown, NY), a competitive chemiluminescent immunoassay. For the traditional CST, a cortisol concentration ≥18 mcg/dL at any time point during the test was used to define normal (negative). Patients with a positive (no results >18 mcg/mL) CST were defined as “screen positives” for the purposes of this analysis. Patient location data were available that allowed for an ICU vs non-ICU comparison.
Statistical analyses were performed in SAS version 9.4 (SAS Institute Inc, Cary, North Carolina). Continuous variables were compared by using a 2-tailed Student t test. Percentiles and proportions were compared by using χ2 tests or Fisher’s exact tests when appropriate. The concordance of screening at each time point compared with the traditional CST was calculated. Positive percent agreement (PPA) with the traditional CST in each subgroup (ICU and floor) and combined was also evaluated. A P value of .05 was used to determine significance.
RESULTS

Cortisol concentrations obtained at 30 minutes were significantly higher than baseline cortisol concentrations (baseline: 12.8 mcg/dL; 30 minutes: 23.9 mcg/dL; P < .001) for all patients. The average cortisol concentrations obtained at 60 minutes (27.4 mcg/dL) were significantly higher than those at baseline and 30 minutes (P < .001). This trend was seen in each subgroup of patients in the ICU and on the floor (Figure). The average baseline cortisol concentration was higher for ICU patients compared to floor patients (17.6 mcg/dL vs 10.9 mcg/dL, respectively).
By using the traditional CST, there were 26 (13.1%) positive tests for AI in ICU patients and 84 (16.7%) positive tests in floor patients (Table).
Only 13% of CSTs were started in the recommended 3-hour window from 6:00
DISCUSSION
Our investigation of 702 CSTs, the largest retrospective analysis to date, finds that the 60-minute cortisol concentration is significantly higher than the 30-minute concentration in a standard, high-dose CST. Sixty-minute cortisol concentrations are more concordant with traditional CST results than the 30-minute concentrations in both critically ill ICU and noncritically ill floor patients. This suggests that a single 60-minute measurement is sufficient for AI screening. The use of only 30-minute concentrations would lead to a significant increase in false-positive screening tests and significantly lower PPA (98% vs 57%). With peak cortisol concentrations occurring at 60-minutes poststimulation, measuring both 30- and 60-minute poststimulation concentrations does not appear to be of significant clinical benefit. The cost-saving from reduced phlebotomy and laboratory expenses would be significant, especially in locations with limited staff or financial resources. Our findings are similar to other recent results by Chitale et al.,17 Mansoor et al.,16 and Zueger et al.18