A Randomized Cohort Controlled Trial to Compare Intern Sign-Out Training Interventions





BACKGROUND: Although previous studies have investigated the efficacy of specific sign-out protocols (such as the illness severity, patient summary, action list, situation awareness and contingency planning, and synthesis by reviewer [I-PASS] bundle), the implementation of a bundle can be time consuming and costly. We compared 4 sign-out training pedagogies on sign-out quality.
OBJECTIVE: To evaluate training interventions that best enhance multidimensional sign-out quality measured by information exchange, task accountability, and personal responsibility.
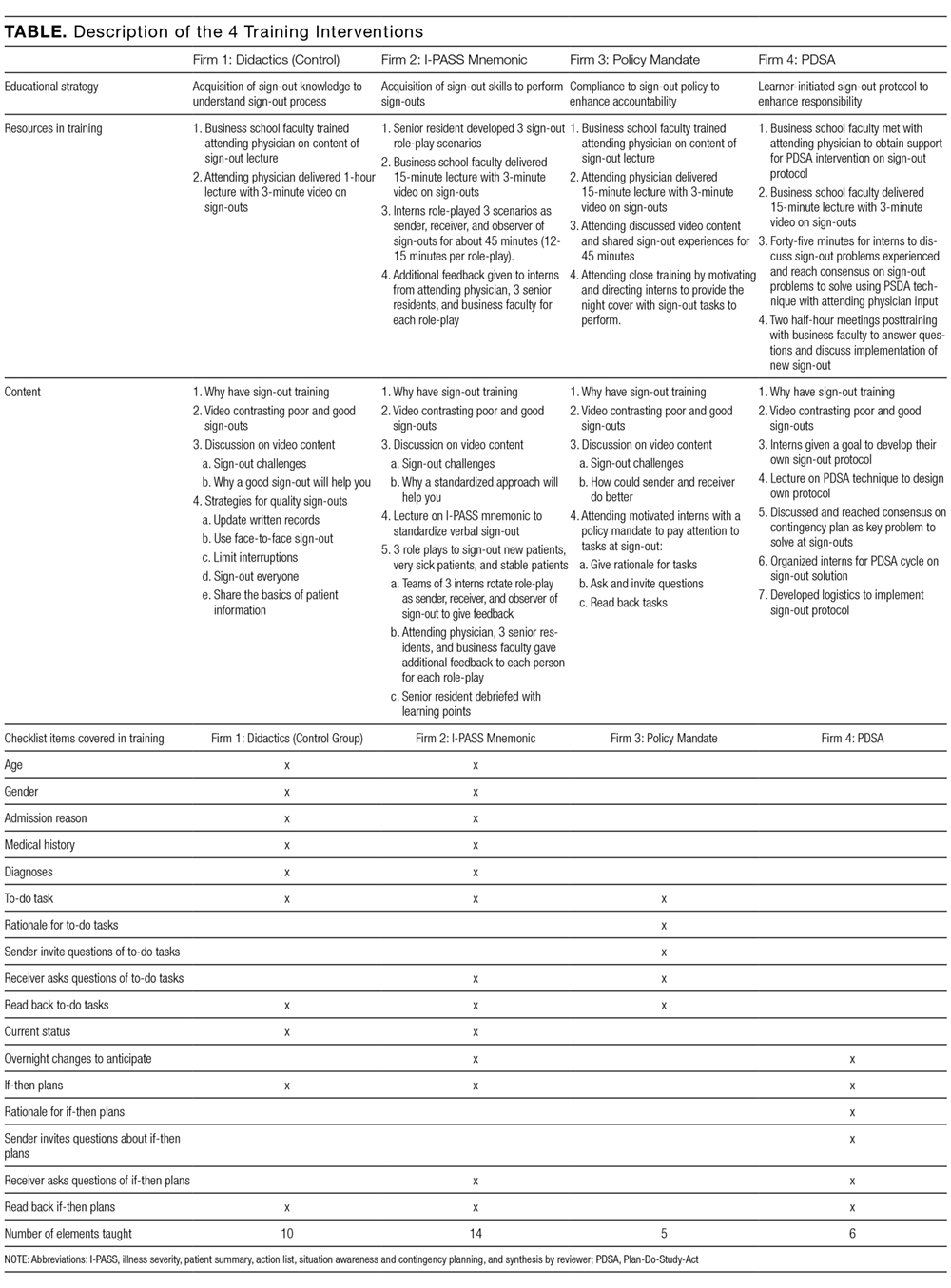
INTERVENTION: Four general internal medicine firms were randomly assigned into 1 of the following 4 training interventions: didactics (control), I-PASS, policy mandate on task accountability, and Plan-Do-Study-Act (PDSA).
SETTING: First-year interns at a large, Mid-Atlantic internal medicine residency program.
MEASUREMENTS: Eight trained observers examined 10 days each in the pre- and postintervention periods for each firm using a standardized sign-out checklist.
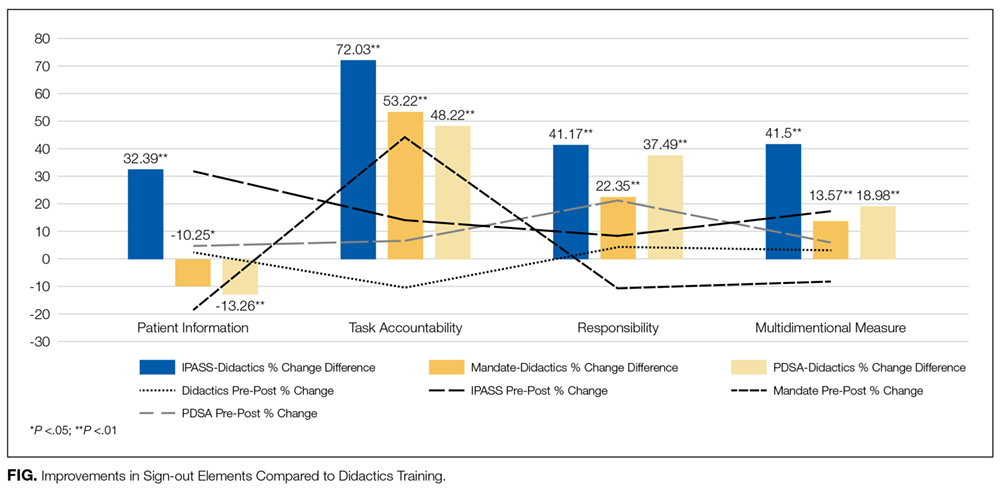
RESULTS: Pre- and postintervention differences showed significant improvements in the transfer of patient information, task accountability, and personal responsibility for the I-PASS, policy mandate, and PDSA groups, respectively, in line with their respective training foci. Compared to the control, I-PASS reported the best improvements in sign-out quality, although there was room to improve in task accountability and responsibility.
CONCLUSIONS: Different training emphases improved different dimensions of sign-out quality. A combination of training pedagogies is likely to yield optimal results.
© 2017 Society of Hospital Medicine
Data Collection Process
Outcomes
We measured improvements in sign-out quality by the mean percentage differences for each of the 3 dimensions of sign-out, as well as a multidimensional measure of sign-out comprising the 3 dimensions for each firm in 2 ways: (1) pre- and postintervention, and (2) vis-à-vis the control group postintervention.
Statistical Analysis
We factor analyzed the 17 sign-out elements using principal components analysis with varimax rotation to confirm their groupings within the 3 dimensions of sign-out using Statistical Package for the Social Sciences (SPSS) version 24 (IBM, North Castle, NY). We calculated the mean percentage differences and used Student t tests to evaluate statistical differences at P < 0.05.
RESULTS
Five hundred and sixty-three patient sign-outs were observed prior to the training interventions (κ = 0.646), and 620 patient sign-outs were observed after the interventions (κ = 0.648). Kappa values derived from SPSS were within acceptable interrater agreement ranges. Factor analysis of the 17 sign-out elements yielded 3 factors that we named patient information, task accountability, and responsibility, as shown in the supporting Table.
DISCUSSION
The results indicated that after only 1 hour of training, skill-based, compliance-based, and learner-initiated sign-out training improved sign-out quality beyond knowledge-based didactics even though the number of sign-out elements taught in the latter 2 was lower than in the didactics group. Different training emphases influenced different dimensions of sign-out quality so that training interns to focus on task accountability or responsibility led to improvements in those dimensions only. The lower scores in other dimensions suggest potential risks in sign-out quality from focusing attention on 1 dimension at the expense of other dimensions. I-PASS, which covered the most sign-out elements and utilized 5 facilitators, led to the best overall improvement in sign-out quality, which is consistent with previous studies.3,12 We demonstrated that only 1 hour of training on the I-PASS mnemonics using video, role-playing, and feedback led to significant improvements. This approach is portable and easily applied to any program. Potential improvements in I-PASS training could be obtained by emphasizing task accountability and responsibility because the mandate and PDSA groups obtained higher scores than the I-PASS group in these dimensions.
Limitations
We measured sign-out quality in the evening at this site because it was at greatest risk for errors. Future studies should consider daytime sign-outs, interunit handoffs, and other hospital settings, such as community or rural hospitals and nonacute patient settings, to ascertain generalizability. Data were collected from observations, so Hawthorne effects may introduce bias. However, we believe that using a standardized checklist, a control group, and assessing relative changes minimized this risk. Although we observed almost 1200 patient sign-outs over 80 shift changes, we were not able to observe every intern in every firm. Finally, no sentinel events were reported during the study period, and we did not include other measures of clinical outcomes, which represent an opportunity for future researchers to test which specific sign-out elements or dimensions are related to clinical outcomes or are relevant to specific patient types.