Helping Seniors Plan for Posthospital Discharge Needs Before a Hospitalization Occurs: Results from the Randomized Control Trial of PlanYourLifespan.org





BACKGROUND: Hospitalized seniors are frequently too sick to make informed decisions about their postdischarge care. Subsequently, loved ones often make support choices (eg, skilled nursing facility placement, caregivers) at discharge. We sought to advance the timeline for postacute care decisions to before a hospitalization occurs.
OBJECTIVE: Investigate the effect of PlanYourLifespan.org (PYL) on knowledge of posthospital discharge options.
DESIGN: Multisite randomized controlled trial.
SETTING/PATIENTS: Nonhospitalized adults, aged ≥65 years, living in urban, suburban, and rural areas of Texas, Illinois, and Indiana.
INTERVENTION: PYL is a national, publicly available tool that provides education on posthospital therapy choices and local home-based resources.
MEASUREMENTS: Participants completed an in-person baseline survey, followed by exposure to intervention or attention control (AC) websites, then 1-month and 3-month telephone surveys. The primary knowledge outcome was measured with 6 items (possible 0-6 points) pertaining to hospital discharge needs.
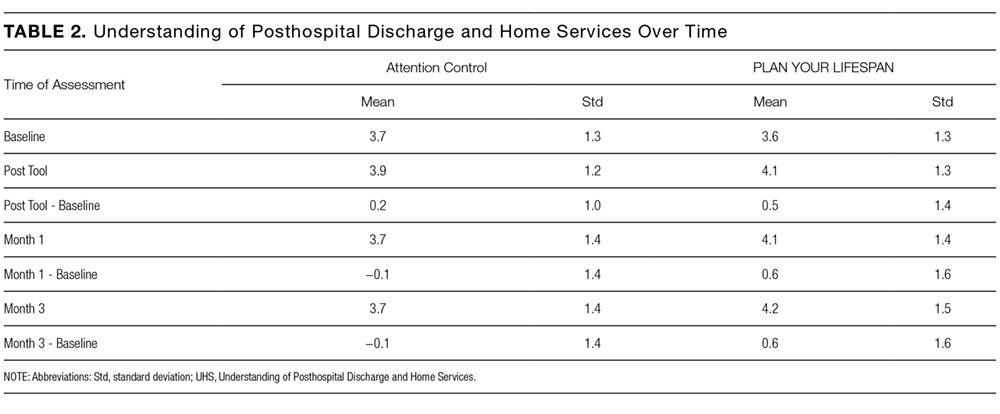
RESULTS: Among 385 participants randomized, mean age was 71.9 years (standard deviation 5.6) and 79.5% of participants were female. At 1 month, the intervention group had a 0.6 point change (standard deviation = 1.6) versus the AC group who had a −0.1 point change in knowledge score. Linear mixed modeling results suggest sex, health literacy level, level of education, income, and history of high blood pressure/kidney disease were significant predictors of knowledge over time. Controlling for these variables, treatment effect remained significant (P < 0.0001).
CONCLUSION: Seniors who used PYL demonstrated an increased understanding of posthospitalization and home services compared to the control group.
TRIAL REGISTRATION: Clinicaltrials.gov Identifier: NCT02256072.
© 2017 Society of Hospital Medicine
RESULTS
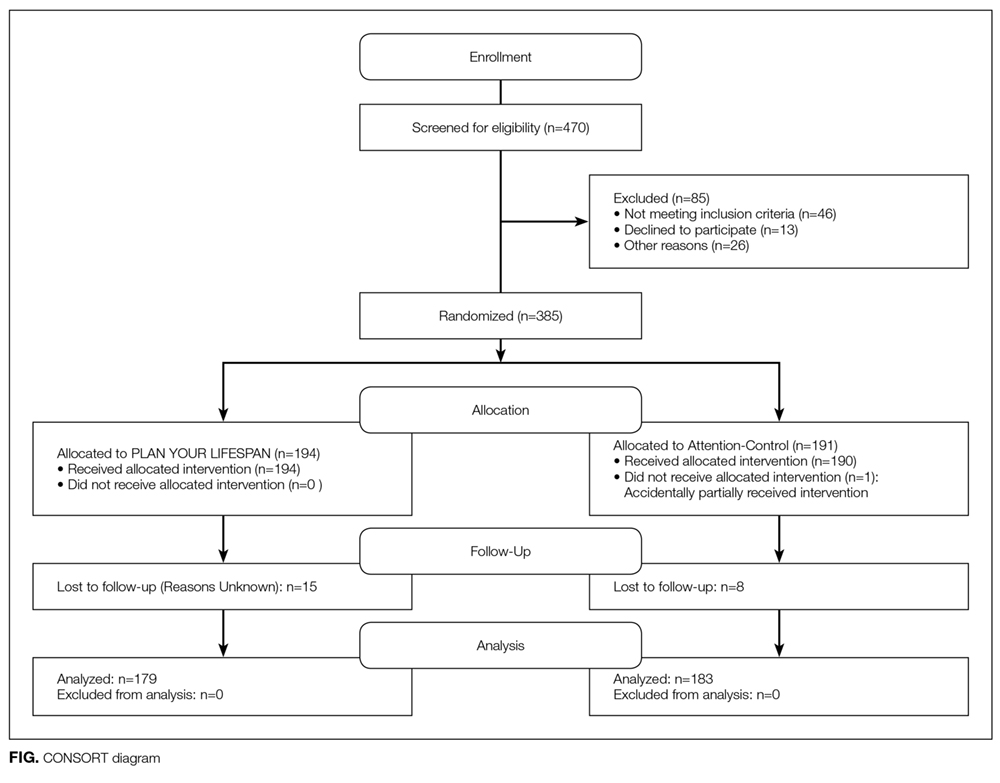
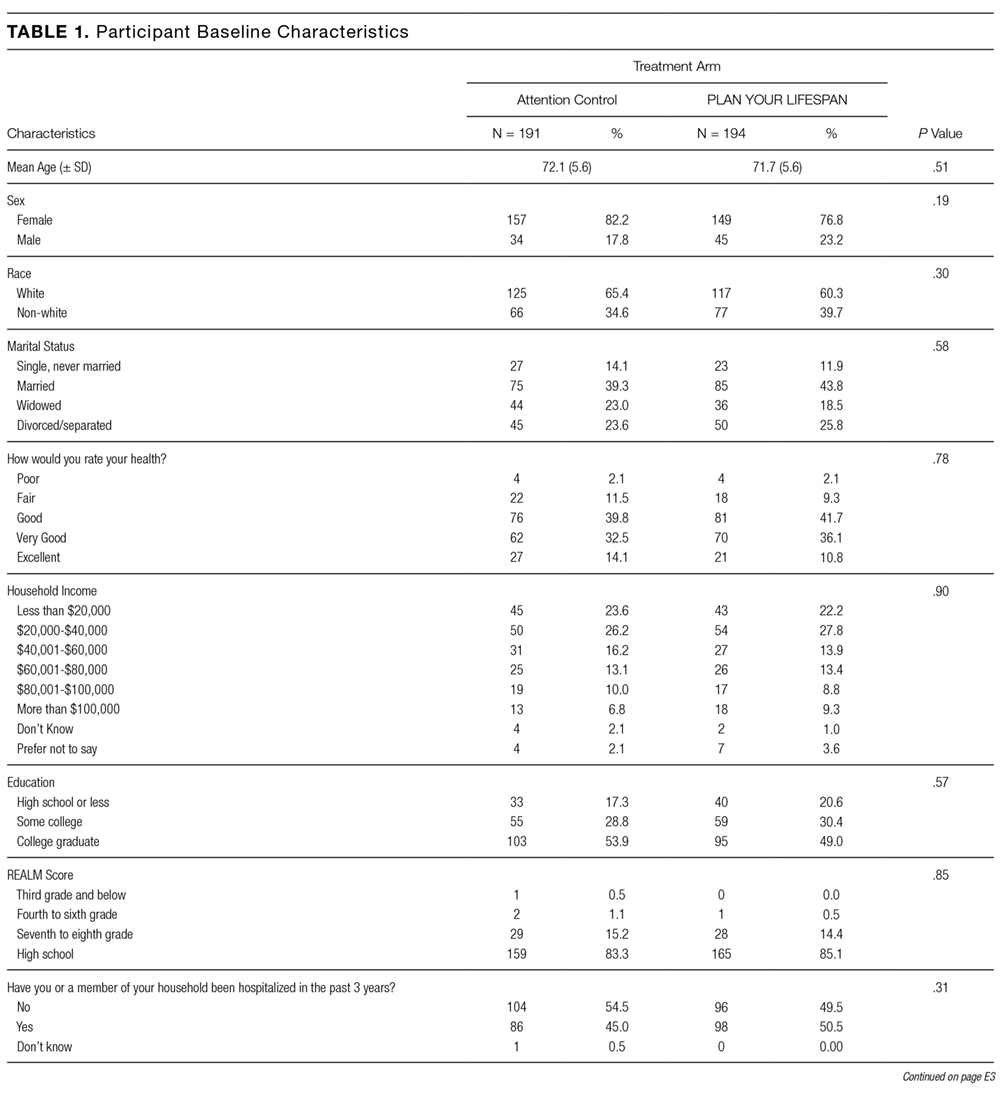
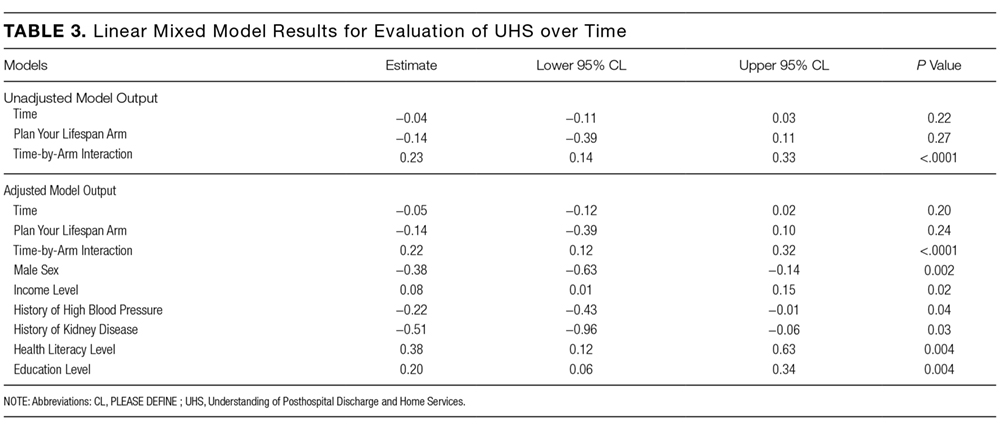
Table 3 illustrates linear mixed model results both failing to adjust and adjusting for potentially influential baseline covariates. In both instances, the interaction term (arm-by-time) was highly significant (P < 0.0001) in predicting UHS score, suggesting that, when compared to the AC arm, the intervention arm exhibited a large mean slope in UHS score over time. That is, understanding home services score tended to increase at a faster rate for those in the active arm. Higher levels of income (P = 0.0191), literacy (P = 0.0036), and education (P = 0.0042) were associated with increased UHS scores; however, male sex (P = 0.0023) and history of high blood pressure (P = 0.0409) or kidney disease (P = 0.0278) were negatively associated with UHS scores.

CONCLUSION/DISCUSSION
The results of our study show that among seniors, PYL improved their understanding of home-based services and the services that may be required following a hospitalization. Educating seniors about what to expect regarding the transition home from a hospital before a hospitalization even occurs may enable seniors and their families to plan ahead instead of reacting to a hospitalization. PYL, a national, publicly available tool with links to local resources may potentially help in advancing transitional discharge care to prior to a hospitalization.
To our knowledge, this is one of the first websites and trials devoted to planning for seniors’ health trajectory as they age into their 70s, 80s, 90s, and 100s. Clinicians regularly discuss code status and powers of attorney during their end-of-life discussions with patients. We encourage clinicians to ask patients, “What about the 10 to 20 years before you die? Have you considered what you will do if you get sick or need help at home?” While not replacing a social worker, the ability of PYL to connect seniors to local resources makes it somewhat of a “virtual social worker.” With many physician practices unable to afford social workers, PYL provides a free-of-charge means of connecting seniors to area resources.
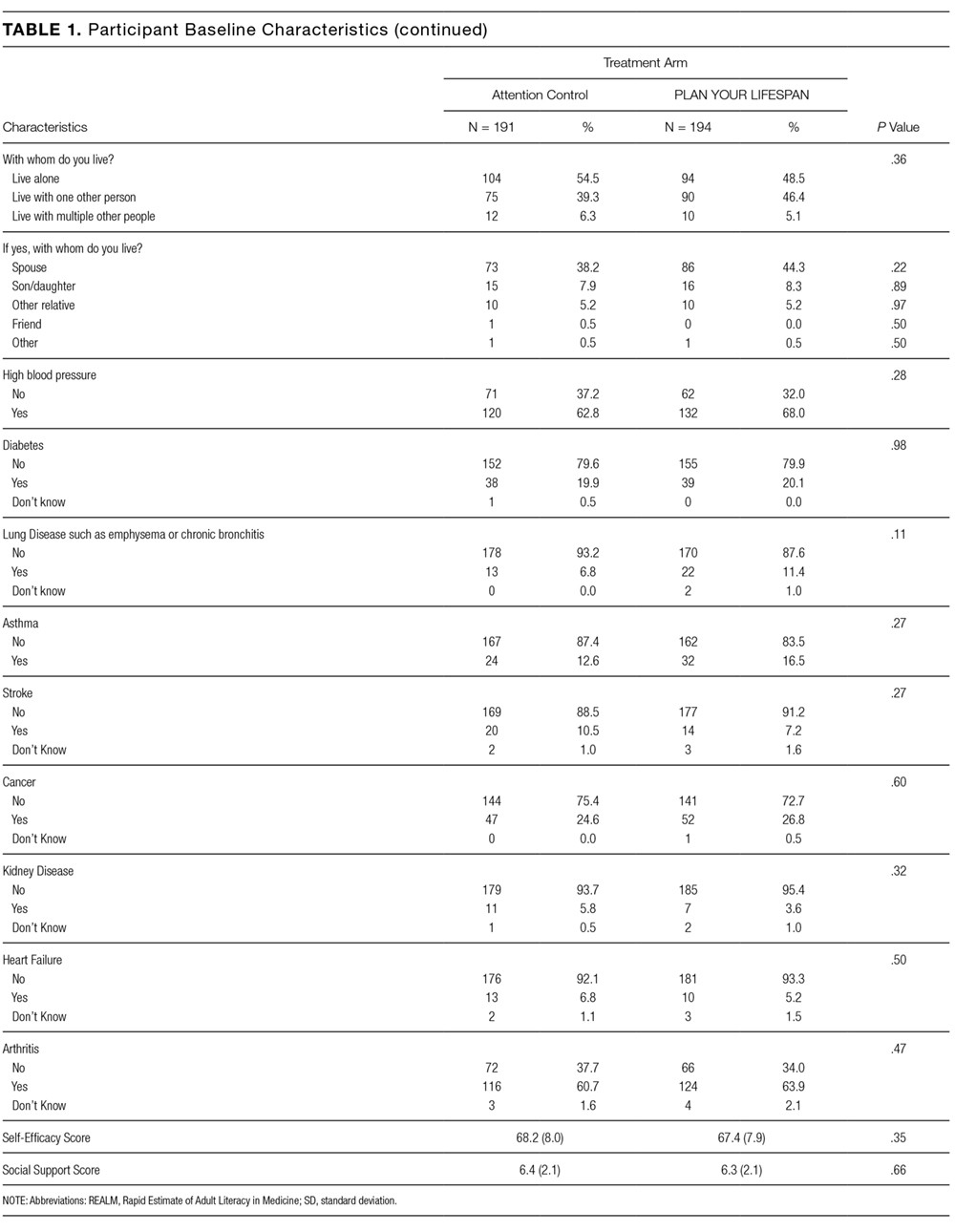
The study participants were in general white, educated, and in reasonably good health. This may be a limitation of this study given that it could impact the generalizability of the study results, as we are unable to know for certain if these same results would be observed with participants who have lower educational levels and are in poor health. Power considerations in this study did not account for comparison of outcomes within specific subgroups so we were unable to assess outcomes in groups such as those with limited health literacy, low social support, or low self-efficacy. The trial was also limited by our inability to collect information on whether or not the knowledge gains observed in the study led to any measureable outcomes. Due to the relatively short follow-up time, we were unable to ascertain whether any study participants were hospitalized during the study follow-up period and if so, if exposure to PYL had any impact on patient anxiety, length of hospital stay, and/or caregiver burden. We were also unable to assess patients’ ability to utilize and carry out their posthospitalization discharge plans if they had one in place. Future studies with longer follow-up are needed to determine these important, measurable outcomes.
Potential implications of planning for a senior’s lifespan are expansive. If hospitalized seniors knew their preferred SNF for subacute rehabilitation on the first day of their hospitalization, hospital lengths of stay could potentially be reduced. If families knew which caregiver agencies, Area Agency on Aging, or Village their senior wished to use, obtaining services would perhaps be easier to accomplish.
