Vascular Ultrasonography: A Novel Method to Reduce Paracentesis Related Major Bleeding





Paracentesis is a core competency for hospitalists. Using ultrasound for fluid localization is standard practice and involves a low-frequency probe. Experts recommend a “2-probe technique,” which incorporates a high-frequency ultrasound probe in addition to the low-frequency probe to identify blood vessels within the intended needle path. Evidence is currently lacking to support this 2-probe technique, so we performed a pre- to postintervention study to evaluate its effect on paracentesis-related bleeding complications. From February 2010 to August 2011, procedures were performed using only low-frequency probes (preintervention group), while the 2-probe technique was used from September 2011 to February 2016 (postintervention group). A total of 5777 procedures were performed. Paracentesis-related minor bleeding was similar between groups. Major bleeding was lower in the postintervention group (3 [0.3%], n = 1000 vs 4 [0.08%], n = 4777; P = 0.07). This clinically meaningful trend suggests that using the 2-probe technique might prevent paracentesis-related major bleeding.
© 2018 Society of Hospital Medicine
DISCUSSION
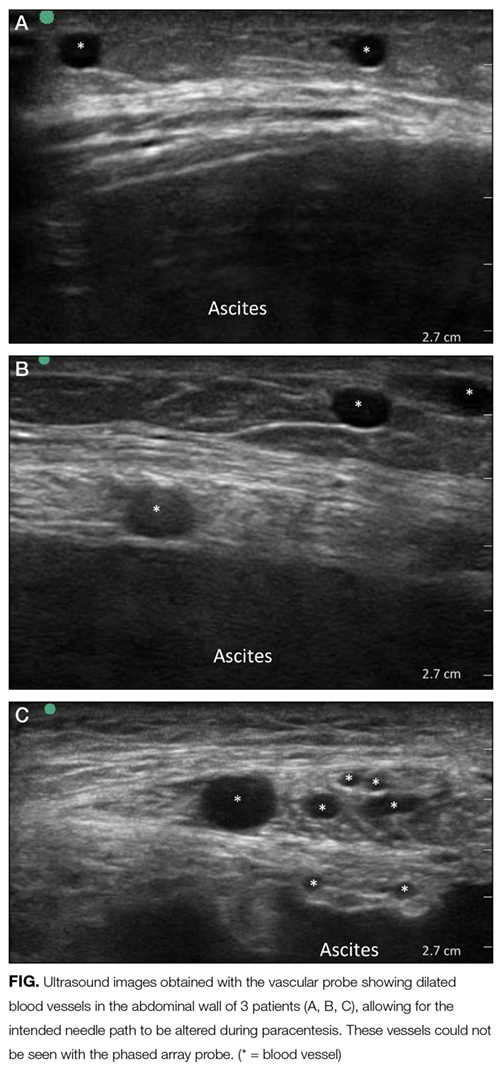
To our knowledge, we report the largest series of paracentesis prospectively evaluated for bleeding complications, and this is the first study to evaluate whether adding a vascular ultrasound (high-frequency probe) avoids major bleeding. In our series, up to 10% of patients had abnormal vessels seen with a vascular ultrasound that were within the original intended trajectory path of the needle. These vessels were also likely present yet invisible when ultrasound-guided paracentesis using only the standard, low-frequency probe was being performed. It is unknown whether these vessels are routinely traversed with the needle, nicked, or narrowly avoided during paracenteses performed using only a low-frequency probe.
Procedure-related bleeding may not be completely avoidable, despite using the vascular probe. Some authors have suggested that the mechanism of bleeding is more related to the rapid reduction in intraperitoneal pressure, which increases the gradient across vessel walls, resulting in rupture and bleeding.6 However, in our series, using vascular ultrasound also reduced major bleeding to numbers lower than those historically reported in the literature (0.2%).3-4 Our preintervention number needed to harm was 333 procedures to cause 1 major bleed, compared to 1250 (or 1666 using the 3-patient bleeding analysis) in the postintervention group. In 2008, 150,000 Medicare beneficiaries underwent paracentesis.13 Using our study analysis, if vascular ultrasound was used on these patients, up to 360 major bleeds may have been prevented, along with a corresponding reduction in unnecessary morbidity and mortality.
Our study has several limitations. First, it was limited to 1 center with 1 very experienced proceduralist. Although it is possible that the reduction in major bleeding may have been due to the increasing experience of the proceduralist over time, we do not think that this is likely because he had already performed thousands of paracenteses over 9 years before the start of our study.
CONCLUSION
Our results suggest that using the 2-probe technique to predetermine the needle path before performing paracentesis might prevent major bleeding. Based on our findings, we believe that the addition of a vascular ultrasound during paracentesis should be considered by all hospitalists.
Acknowledgments
The authors acknowledge Drs. Douglas Vaughan and Kevin O’Leary for their support and encouragement of this work. They would also like to thank the Cedars-Sinai Enterprise Information Systems Department for assistance with their data query.
Disclosure
The authors have no relevant financial disclosures or conflicts of interest to report.