Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Journal of Hospital Medicine 12(5). 2017 May;301-309 | 10.12788/jhm.2730
Antimicrobial stewardship programs (ASPs) have been advocated to improve antimicrobial utilization, but program implementation is variable.
Objective
To determine associations between ASPs and facility characteristics, and inpatient antimicrobial utilization measures in the Veterans Affairs (VA) system in 2012.
Design
In 2012, VA administered a survey on antimicrobial stewardship practices to designated ASP contacts at VA acute care hospitals. From the survey, we identified 34 variables across 3 domains (evidence, organizational context, and facilitation) that were assessed using multivariable least absolute shrinkage and selection operator regression against 4 antimicrobial utilization measures from 2012: aggregate acute care antimicrobial use, antimicrobial use in patients with non-infectious primary discharge diagnoses, missed opportunities to convert from parenteral to oral antimicrobial therapy, and double anaerobic coverage.
Setting
All 130 VA facilities with acute care services.
Results
Variables associated with at least 3 favorable changes in antimicrobial utilization included presence of postgraduate physician/pharmacy training programs, number of antimicrobial-specific order sets, frequency of systematic de-escalation review, presence of pharmacists and/or infectious diseases (ID) attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist. Variables associated with 2 unfavorable measures included bed size, the level of engagement with VA Antimicrobial Stewardship Task Force online resources, and utilization of antimicrobial stop orders.
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
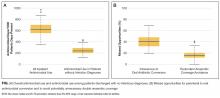
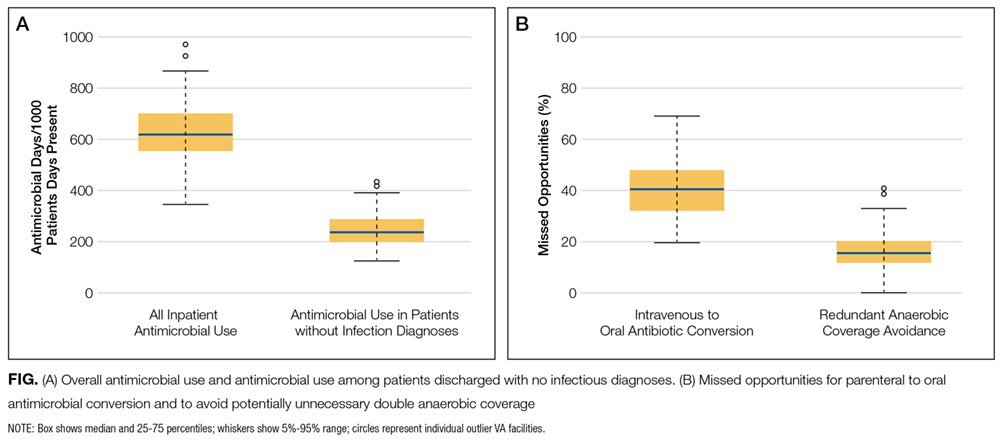
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).






")

")