Reducing hospital readmissions through primary care practice transformation





This study found that a “culture of continuity” using processes that strengthen outpatient-inpatient caregiver communication improves patient care.
METHODS
Study setting and preintervention practice routines in 2 patient groups
The study setting for Group 1 involved patients with assigned primary care providers (PCPs) in a university-based practice group at 4 outpatient clinics. The study setting for Group 2 included patients with assigned PCPs from county and community health centers, involving 12 primary care clinics in total. While the groups’ patient populations were distinguished for descriptive purposes, in practice the patients were admitted to the same inpatient treatment teams and university-based hospital in a metropolitan setting. For both groups, the primary care practices admitted patients to the hospital directly from clinic or through the emergency department (ED).
An admitting team from one of the inpatient services completed the admission, initiated treatment, and discharged patients. Preintervention, limited discharge case management occurred at the hospital, driven primarily by the treating team’s requests. The admitting team also attempted to schedule outpatient follow-up appointments with an available PCP at the patient’s primary clinic after discharge. Obstacles to successful appointment scheduling prior to discharge included but were not limited to discharges over weekends or holidays or after clinic hours. Additionally, for both groups, discharge summaries were sent to the PCP either electronically via the electronic medical record (EMR) or via system-generated automated fax.
Creating a culture of continuity in Group 1
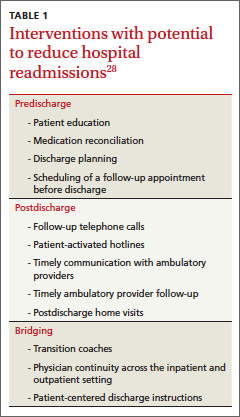
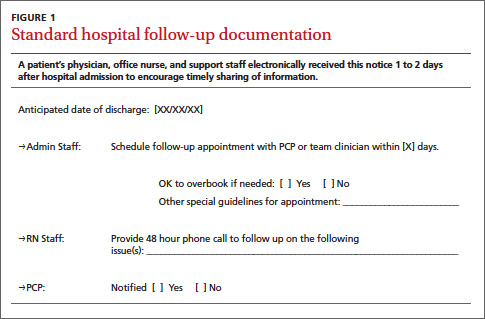
Transformation of outpatient activities. We developed several important processes to transform the patient experience through hospitalization and discharge. Together, these processes created a “culture of continuity” to prevent avoidable readmissions. We introduced an innovative, systematic approach to notifying the clinic and primary care clinician about initial admission. We also gave notification immediately upon discharge, rather than waiting until after discharge, as had been occurring. This patient-centered change engaged the primary care team in the care of the patient while hospitalized and during discharge planning; it actively ensured that follow-up appointments occurred within 1 week after discharge. Prior to this intervention, there was no system for ensuring timely follow-up after hospital discharge. The new expectation for the ambulatory clinics was that clinic staff could “reach in” to the patient during the hospital stay and actively contact the patient before discharge to schedule a postdischarge appointment at the patient’s convenience.
The 4 practices had embraced and implemented the PCMH model, a core component of which is care coordination.34,35 Each clinic appointed a registered nurse (RN) to serve as a team-based care manager (CM) for patients being discharged from the hospital. Responsibilities included fielding calls or electronic communications from the inpatient team, developing a hospital follow-up workflow, developing a standardized list of questions to ask each patient after discharge, and calling patients to ensure a follow-up appointment was scheduled, ideally within 2 to 3 days and at least within 7 days of discharge. The CM prioritized scheduling follow-up appointments with the patient’s PCP to ensure the highest level of continuity.
In addition to patient-specific documents, CMs received electronic reports from inpatient teams (including from the ED, medical and surgical intensive care units, and surgery) listing all Group 1 patients discharged from the hospital. Reports were run daily and allowed the outpatient clinic staff and CMs to verify patients against previous lists of anticipated discharges, and to generate their own lists. The CMs would then make follow-up phone calls and ensure that appointments were scheduled for these patients.
Medical directors at the 4 clinics received monthly summary reports profiling clinical activities related to hospitalizations. A data team (led by author SF) created the reports, which initially focused on care delivered in ambulatory settings (and included the development of a “balanced scorecard” to assess quality of care, financial productivity, and operational efficiency36). The data team developed new reports specifically for hospital admissions, discharges, and readmissions, identifying:
• all patients admitted by inpatient team
• the number and percentage of patients who were readmitted within 30 days
• the number and percentage of patients who had received a follow-up phone call or electronic communication from the outpatient team
• the number of patients who had follow-up visits after discharge within 7 and 30 days
• the number of patients who had clinic visits prior to readmission
• all patients discharged from any service within the prior 24 hours.
These reports, which had patient drilldown capability, were forwarded to all providers and teams at each clinic by the medical director. Teams at each clinic were then charged with analyzing the readmissions, identifying high-risk patients, and improving the coordination of care for these patients, including the use of RN/clinician co-visits and proactive outreach from the team-based nurses and staff.