Management of the low-grade abnormal Pap smear: What are women’s preferences?





- OBJECTIVE: To evaluate preferences among ethnically diverse women for the management of a low-grade abnormal Pap smear result: early colposcopy or observation with repeat Pap smears.
- STUDY DESIGN: Structured interviews were conducted with 170 women of diverse ethnic backgrounds to assess their preferences. Trained personnel conducted standardized interviews. A standard description of all tests and procedures was read to participants. The participants were presented with scenarios of contrasting management approaches for a hypothetical low-grade abnormal Pap smear result—observation with repeat Pap smear vs. immediate colposcopy.
- POPULATION: Study participants were recruited from the waiting rooms of 5 family planning clinics in Northern California’s Central Valley.
- OUTCOMES MEASURED: The primary outcome measures for each scenario were utilities (quantified preferences for specific health states) measured by the Standard Gamble.
- RESULTS: The range in utilities was large for all scenarios. Mean utilities (SD) for observation: 0.96 (± 0.13) followed by resolution; 0.93 (± 0.17) followed by cryotherapy; 0.91 (± 0.21) followed by cone biopsy. Mean utilities for early colposcopy: 0.93 (± 0.20) followed by resolution; 0.95 (± 0.14) followed by cryotherapy; and 0.92 (± 0.16) followed by cone biopsy. Subject characteristics explained less than 20% of the variance in utilities. Decision analysis gave a slightly higher overall utility for early colposcopy (0.940 vs 0.932 for observation), but was sensitive to small changes in branch utilities.
- CONCLUSIONS: Women’s preferences for management of a low-grade abnormal Pap result vary widely. Clinicians should adopt a flexible approach to the management of low-grade abnormal Pap smears to incorporate individual preferences.
The decision model with baseline probabilities is shown in Figure 1. The model was simplified to exclude the outcome of cervical cancer, which is a very rare outcome for women with ASC or LSIL cervical smears who have adequate follow-up.5 In the baseline analysis, the overall utility of early colposcopy was slightly favored over the overall utility of the observation approach (utility of observation = 0.932; utility of early colposcopy = 0.940).
Sensitivity analysis examines the effect of varying elements of the model on the outcome. In sensitivity analyses of probabilities, the early colposcopy branch was favored, but the differences were small. The maximum difference in utilities between branches was 0.012 in these sensitivity analyses. In 1-way sensitivity analysis of branch utilities, threshold utility values to favor the observation branch were 0.986 for spontaneous resolution after observation and 0.898 for early colposcopy. Threshold values for cryotherapy were 0.938 for observation and 0.938 for early colposcopy.
TABLE 2
Characteristics of study subjects (n = 170)
| Characteristics | n (%) |
|---|---|
| Mean age (range), y | 26 (14–53) |
| Education | |
| Less than high school | 58 (34%) |
| High school | 77 (45%) |
| Some college | 35 (20%) |
| Ethnicity | |
| African American | 21 (12%) |
| Caucasian | 84 (49%) |
| Latina | 46 (27%) |
| Other | 21 (12%) |
| Interview language, Spanish | 15 (9%) |
| Prior colposcopy | 23 (14%) |
| Moderately or very religious | 64 (38%) |
| Knows someone with cervical cancer | 43 (25%) |
TABLE 3
Adjusted standard gamble values and paired differences* (n=148)
| Management Strategy | ||||
|---|---|---|---|---|
| Short-term outcome | Observation Mean (SD) | Early colposcopy Mean (SD) | Difference | P value (2 sided) |
| Spontaneous resolution | .96 ±..13) | .93±.20) | .03 ±..15) | .01 |
| Cryotherapy | .93 ±..17) | .95 ±..14) | -.02 ±.11) | .02 |
| Cone biopsy | .91 ±..21) | .92 ±..16) | -.02 ±..17) | .23 |
| *Adjusted to scale so that immediate death had a utility of 0 and “full health with all normal Pap smears” had a utility of 1. | ||||
FIGURE 1Decision model comparing observation with early colposcopy *
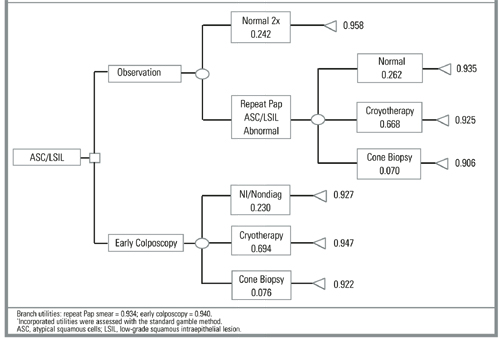
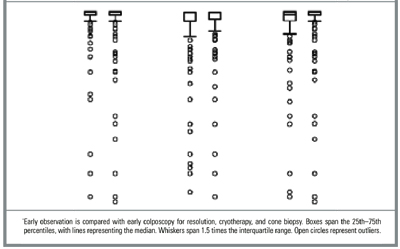
FIGURE 2Distribution of individual utilities as assessed by the standard gamble*
Discussion
We found wide variation in women’s preferences for management approaches to a low-grade abnormal Pap smear result. The range of responses was very large and the variation between individuals rating the same scenario was substantially greater than the variation in mean ratings between different scenarios. Measured subject characteristics explained only a small proportion of the observed variation, indicating that other unmeasured factors contributed substantially to the variation. Although 25% of subjects stated they knew someone with cervical cancer, this high percentage seems improbable and more likely reflects knowledge of someone who had an abnormal Pap smear.
The decision model displayed a small preference for immediate colposcopy. This may be related to preference for quicker resolution of the concern about cancer, although it involves more procedures. Small changes in utilities for spontaneous resolution and cryotherapy influenced the model to prefer observation. For cryotherapy, these utility values were within 1 standard deviation of the mean.
Our finding of a wide variation in preferences is supported by other patient preference studies,12-14 including 2 on this subject. Ferris et al assessed triage preferences for the evaluation and management ASC and LSIL.13 They used a questionnaire with a sample of 968 women who presented for care at obstetrics and gynecology and family practice clinics. They found that more women preferred repeat Pap smear when the index smear was ASC, and more women preferred colposcopy when the index smear was LSIL. Among a group of 136 Canadian women with atypia or LSIL referred for colposcopy, Meana et al found that 64% preferred early colposcopy, while 17% preferred observation and 17% had no strong preference.14
The factors contributing to patient preferences are complex. Differences in preferences may be influenced by knowledge and understanding of the disease and possible interventions, risk aversion, access to services, socioeconomics, cultural background, and other factors. While 1 patient may be most interested in establishing a definitive diagnosis and undergoing treatment as soon as possible, another may place priority on avoiding invasive or uncomfortable procedures. How differences in patient preferences influence clinical choices is highlighted by the work of Kuppermann et al.15 These investigators found that utilities for outcomes of prenatal diagnostic testing predicted subsequent testing behavior.
Our findings are limited by our use of a convenience sample of women attending family planning clinics. They may not be representative of women’s preferences in general, or even those of women attending family planning clinics. Outcomes in our study were specified during the preference assessment process; in real decision making, the outcome is always unknown at the time the decision is made. We did not include HPV typing as an option in our clinical scenarios. While HPV typing may have a role for triage of ASC,6,16 it appears not to be useful in management of LSIL.17
Cost-effectiveness analysis would offer important information about which management approach might be favored in the context of resource allocation. For decision making by individual patients and doctors, however, decision analysis is often more relevant. In this case, the “preferred” decision is very sensitive to patient utilities, emphasizing the need for clear physician-patient communication.