Hand compression neuropathy: An assessment guide





When a patient presents with pain or paresthesias of the hand and fingers, knowing what to ask, what to look for, and which tests to consider is essential.
Pronator syndrome
Pronator syndrome (PS) is a proximal median neuropathy that may present in isolation or in combination with CTS as a double crush syndrome. Clinical symptoms include features of CTS and sensory paresthesias in the palm and distal forearm in the distribution of the palmar cutaneous branch of the median nerve. PS is commonly associated with volar proximal forearm pain exacerbated by repetitive activities involving pronation and supination.
PS is not easy to assess. Palpatory examination of a large supracondylar process at the distal humerus proximal to the medial epicondyle on its anteromedial aspect can be difficult, especially if the patient is overweight. And motor weakness is not a prominent feature. What’s more, power assessment of the pronator teres, flexor carpi radialis, and flexor digitorum superficialis may exacerbate symptoms.
Because the symptoms of PS and CTS may be the same, PS provocation maneuvers should be performed on patients with CTS symptoms and paresthesia involving the palm. Start by testing for Tinel’s sign over the pronator teres muscle, although this has been found to be positive in less than 50% of PS cases.17 Palpate the antecubital fossa and the proximal aspect of the pronator teres muscle to assess for discomfort or tenderness.
Pronator compression test. The pronator compression test has been found to be the most sensitive way to assess PS.18,19 This test involves direct compression of the proximal and radial edge of the pronator teres muscle belly along the proximal volar forearm with the thumb.20 It is performed bilaterally on supinated upper extremities, with the clinician applying pressure on each forearm simultaneously (FIGURE 2). If the symptoms in the hand are reproduced in ≤30 seconds, the test is positive. In a study of 10 patients with surgically confirmed PS, the pronator compression test was positive in every case.20,21

Resistance testing. You can also evaluate the pronator teres compression site by testing the patient’s ability to resist pronation with his or her elbow extended and the forearm in neutral position. To test for compression from the bicipital aponeurosis, ask the patient to flex the elbow to approximately 120° to 130° and apply active supinated resistance.22 Likewise, resistance of the long finger proximal interphalangeal joint (IPJ) to flexion—a maneuver performed with elbow fully extended—assesses compression from the fibrous arcade of the flexor digitorum superficialis (FDS).21 A positive resistance test will reproduce the reported symptoms.
Ulnar tunnel syndrome
Symptoms of UTS, which is much less common than CTS, include pain in the wrist and hand that is associated with paresthesia or numbness in the small finger and ulnar half of the ring finger. Patients may report difficulty with motor tasks involving grip and pinch strength or fatigue with prolonged action of the intrinsic muscles. Many also report an exacerbation of symptoms associated with increased wrist flexion or at night.
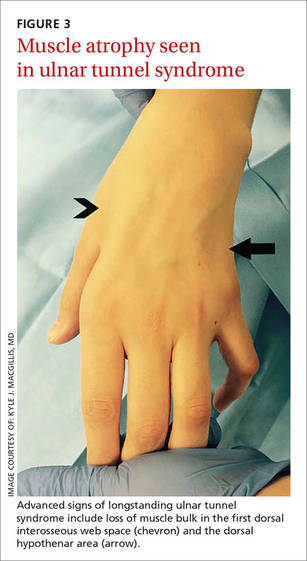
Evaluation of UTS requires a full assessment of the upper extremity, starting with observation of hand posture and muscle bulk to identify signs of chronic nerve compression. The contralateral extremity serves as a control to the neuropathic hand. Classically, chronic ulnar nerve compression leads to intrinsic muscle atrophy, evidenced by loss of topographical soft tissue bulk in the first dorsal web space, the palmar transverse metacarpal arch, and the hypothenar area.23 Ulnar motor nerve dysfunction is limited to the intrinsic muscles of the hand. The inverted pyramid sign, signified by atrophy of the transverse head of the adductor pollicis, is another visual aberrancy,24 as is clawing of the ring finger and small finger. The clawing, which involves hyperextension of the MCPJ and flexion of the proximal and distal IPJ, is commonly known as Duchenne’s sign. FIGURE 3 demonstrates hypothenar atrophy and the loss of muscle bulk in the first dorsal web space.
When you suspect UTS, palpate the wrist and hand in an attempt to locate a mass or area of tenderness. Not all patients with a volar ganglion cyst responsible for UTS present with a palpable mass, but tenderness along the radial aspect of the pisiform or an undefined fullness in this area may be noted.25 Any patient with a palpable mass should be tested for Tinel’s sign over the mass and undergo a thorough vascular assessment. Fracture of the hook of the hamate is indicated by tenderness in the region approximated by the intersection of Kaplan’s line and the proximal extension line from the ring finger.
Perform 2-point discrimination testing at the palmar distal aspect of the small finger and ulnar half of the ring finger. This tests the superficial sensory division of the ulnar nerve that travels within Guyon’s canal. Testing the dorsal ulnar cutaneous nerve involves the skin of the dorso-ulnar hand and dorsum of the long finger proximal to the IPJ. If this area is spared and the palmar distal ulnar digits are affected, compression within Guyon’s canal is likely. If both areas are affected, suspect a more proximal compression site at the cubital tunnel, as the dorsal ulnar cutaneous nerve branches proximal to Guyon’s canal.26
Ulnar motor nerve dysfunction in UTS is limited to the intrinsic muscles of the hand. Assessment of intrinsic muscle function is described in TABLE 3.27-32 It is important to become familiar with the tests and maneuvers described, but also to be aware that a comprehensive evaluation of ulnar nerve motor function requires a combination of tests.
Cubital tunnel syndrome
Cubital tunnel syndrome—the second most common peripheral neuropathy8—involves the proximal site of ulnar nerve compression in the upper extremity. Patients typically report symptoms similar to those of UTS, with sensory paresthesia in the ulnar digits and intrinsic weakness. To learn more about the symptoms, ask if the onset of pain or paresthesia is related to a particular elbow position, such as increased elbow flexion.
Notably, pain is usually not the initial complaint, unless the disease is advanced. This may be the reason atrophic intrinsic changes are 4 times more likely to be seen in patients with cubital tunnel syndrome than in those with CTS.33 You’re more likely to hear about vague motor problems, including hand clumsiness and difficulty with fine coordination of the fingers.34 Thus, it is important to evaluate patients for concurrent UTS and/or CTS, as well as for differentiation.