
Marriage predicts for survival in patients with stage III non–small-cell lung cancer





Background Comprehensive anal
Objective To evaluate whether marital status is an independent predictor of clinical outcomes in patients with stage III NSCLC who are treated uniformly with curative intent.
Methods The Kaplan-Meier method and Cox proportional hazards model were used to estimate the overall survival and freedom from recurrence (FFR) in 355 patients with stage III NSCLC who were treated during 2000-2013.
Results 52% of patients in the cohort were married and were more likely to self-identify as white (P < .0001), reside in zip codes with a higher household median income (P < .0001), have Eastern Cooperative Oncology Group Performance Status of 0 (P = .001), have higher pretreatment albumin (P = .009), undergo surgery (P = .001), and have insurance (P = .029). On multivariate analysis, marital status remained an independent predictor of survival and was associated with a 40% decreased risk of death (P < .0001), further stratifying outcomes beyond gender and stage grouping. FFR was comparable between the 2 groups (P = .108).
Limitations Retrospective analysis; information on individual support system beyond the marital and insurance status and zip code income was not available.
Conclusions In a cancer such as NSCLC, in which modern therapeutic approaches have yielded only modest survival improvements despite considerable treatment-related toxicity, marital status remains an independent predictor for survival. Marriage is likely a surrogate for better psychosocial support; the scale of survival improvements seen justifies investments into supportive care interventional strategies to help advance overall outcomes.
Funding/sponsorship None
Accepted for publication September 6, 2018
Correspondence
Melissa AL Vyfhuis, MD, PhD; mvyfhuis@umm.edu OR
Josephine L Feliciano, MD; jfelici4@jhmi.edu
Disclosures: The authors report no disclosures/conflicts of interest.
Citation JCSO 2018;16(5):e194-e201
©2018 Frontline Medical Communications
doi https://doi.org/10.12788/jcso.0427
We used the Pearson chi-square test to compare categorical variables. OS was calculated from the date of diagnosis (by biopsy of either primary tumor or mediastinal nodes) to the time of death or date of last follow-up. Patients were only censored if they were lost to follow-up. FFR was determined by the date of diagnosis to the time of first failure, with either distant or locoregional disease progression. For this analysis, patients were censored at the time of their last follow-up or death. The Kaplan-Meier product limit method was used to estimate OS and FFR, and we applied the log-rank test to compare outcomes between the 2 cohorts.
We conducted the multivariate analyses using Cox regression with forward model selection. Variables analyzed included age (<60 vs ≥60 years), sex, race (black vs nonblack), median household income, insurance status (Yes vs No), Eastern Cooperative Oncology Group Performance Status (ECOG PS) (range: 0-3; 0 = fully active and 3 = capable of limited self-care, confined to bed/chair >50% of day) at time of diagnosis (0 vs ≥1), pre-CRT BMI, smoking (pack-years), chronic obstructive pulmonary disorder (Yes vs No), Charlson Comorbidity Index score (≤6 vs >7; range, 3-15; this score takes into consideration age, cardiovascular disease, malignancy, and other chronic conditions to calculate 1-year mortality), histology, calculated pretreatment NLR (as a continuous variable), pretreatment albumin (as a continuous variable), T stage, N stage, overall stage (IIIA vs IIIB), radiation technique (3D-CRT vs intensity-modulated radiation therapy [IMRT]), date of diagnosis (divided into quartiles based on proportion diagnosed by years: 2000-2002, 2003-2005, 2006-2009, 2010-2013), use of trimodality therapy, and consolidation chemotherapy. SPSS software (version 23.0) was used for statistical analysis (IBM Corp, Armonk, NY).
Results
Treatment cohorts
Table 1 compares and summarizes patient demographics, disease, and treatment characteristics for married (n = 185; 52.1%) and nonmarried (n = 170; 47.9%) patients. Married patients were more likely to self-identify as being white (P < .0001), reside in zip codes with a higher household median income (P < .0001), have an ECOG PS of 0 (P = .001), have a higher distribution of pretreatment albumin levels (P = .009), and undergo trimodality therapy (P = .001), and they were twice as likely to have insurance (P = .029). Both cohorts were evenly distributed in terms of T stage, N stage, and overall staging. There was no difference in pretreatment NLR or pretreatment BMI between married and single patients. Concurrent CRT was used in more than 85% of patients in both groups, with approximately two-thirds also receiving consolidation chemotherapy (Table 1). Median delivered radiation dose was 64.8 Gy (range, 10.8-81.6 Gy). There was no statistically significant difference in radiation dose delivered to either group, with nearly 90% of the cohort receiving ≥60 Gy.
,

OS and FFR
With a median follow-up of 15 months for all patients and 89 months for surviving patients (range, 1-184 months), married patients had improved OS when compared with the single cohort, with a median survival of 29.6 and 18.4 months, respectively (unadjusted hazard ratio [HR] of married vs nonmarried, .640; 95% confidence interval [CI], 0.502-0.816; P < .0001; Figure 1A). The estimated 2- and 5-year OS for married and single patients were 56% and 31% and 38.6% and 15%, respectively. When stratified by stage, married patients with stage IIIB disease (median survival, 25 months; Figure 1B) had a similar survival to unmarried patients with stage IIIA disease (median survival, 24 months; Figure 1B).
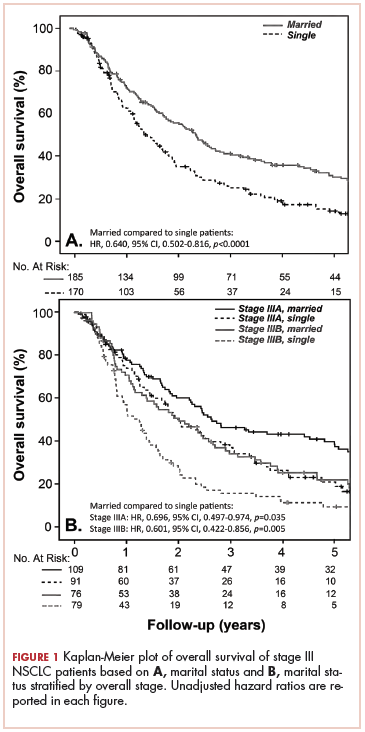
In stage IIIA patients, marital status was associated with an unadjusted HR of .696 (95% CI, 0.497-0.974; P = .035), with a larger OS benefit seen in the IIIB group (unadjusted HR, .601; 95% CI, 0.422-0.856; P = .005).
