Trauma-Informed Telehealth in the COVID-19 Era and Beyond





Background: The Veterans Health Administration (VHA) entered the COVID-19 pandemic crisis with an existing and robust telehealth program, but it still faces a fundamental paradigm shift as most routine outpatient in-person care was converted to telehealth visits. Veterans are a highly trauma-exposed population, and VHA has long offered effective telemental health services. Natural disasters and pandemics like COVID-19 are known to be traumatic. Those with preexisting trauma exposure and mental health conditions are often at greater risk than the general population for long-term adverse health sequelae. Application of trauma-informed principles to telehealth care is critical and timely.
Observations: Trauma-focused care (including telemental health) refers to evidence-based treatment models that directly facilitate recovery from trauma-related conditions like posttraumatic stress disorder. Despite the widespread availability of trauma-focused treatment in VHA, not all veterans chose to engage in it. In contrast, trauma-informed care (TIC) is a global, “universal precautions” approach to providing strengths-based, collaborative quality medical care in any discipline or location. In this article the authors, all primary care and mental health clinicians at VHA, advocate for the application of the 6 Substance Abuse and Mental Health Services Administration principles of trauma-informed care to telehealth. Using examples from telehealth research conducted in trauma-exposed patient populations, we illustrate the characteristics of telehealth that are well suited to delivery of trauma-informed care and suggest readily applicable strategies that can be used across disciplines including primary care and medical/surgical specialties. A primary care patient case scenario is included to illustrate how telehealth visits can be trauma-informed.
Conclusions: Telehealth expansion has occurred nationally out of necessity during the COVID-19 pandemic. Trauma-informed virtual care has the potential to ensure and even expand continuity of medical care by fostering safe and collaborative interactions between patients and the health care team.
Trauma-Informed Telehealth
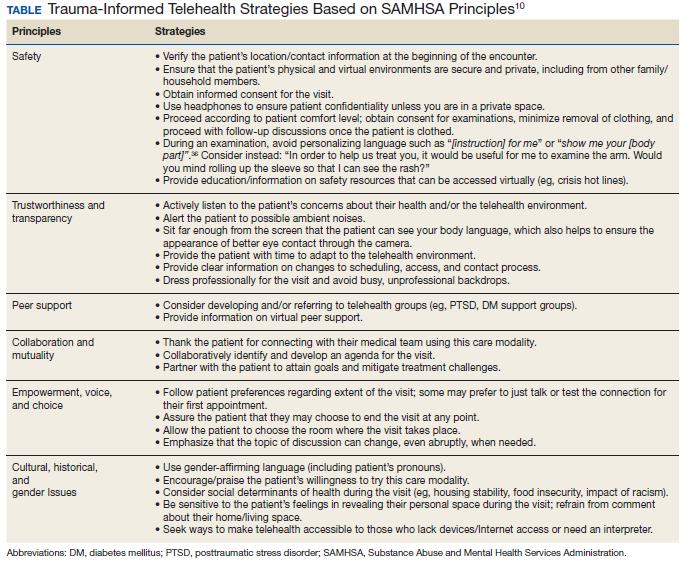
We have discussed how telehealth’s greater flexibility may create an ideal environment in which to implement principles of TIC. It may allow increased collaboration and closeness between patients and clinicians, empowering patients to codesign their care.31,33 The Table reviews 6 core SAMHSA principles of TIC and offers examples of their application to telehealth visits. The following case illustrates the application of trauma-informed telehealth care.
Case Presentation
S is a 45-year-old male veteran of Operation Enduring Freedom (OEF) who served as a combat medic. He has a history of osteoarthritis and PTSD related to combat experiences like caring for traumatic amputees. Before the pandemic began, he was employed as a server at a local restaurant but was laid off as the business transitioned to takeout orders only. The patient worked near a VA primary care clinic and frequently dropped by to see the staff and to pick up prescriptions. He had never agreed to video visits despite receiving encouragement from his medical team. He was reluctant to try telehealth, but he had developed a painful, itchy rash on his lower leg and was concerned about getting care.
For patients like S who may be reluctant to try telehealth, it is important to understand the cause. Potential barriers to telehealth may include lack of Internet access or familiarity with technology, discomfort with being on video, shame about the appearance of one’s home, or a strong cultural preference for face-to-face medical visits. Some may miss the social support benefit of coming into a clinic, particularly in VHA, which is designed specifically for veteran patients. For these reasons it is important to offer the patient a choice and to begin with a supportive phone call that explores and strives to address the patient’s concerns about videoconferencing.
The clinic nurse called S who agreed to try a VVC visit with gentle encouragement. He shared that he was embarrassed about the appearance of his apartment and fearful about pictures being recorded of his body due to “a bad experience in my past.” The patient was reassured that visits are private and will not be recorded. The nurse also reminded him that he can choose the location in which the visit will take place and can turn his camera off at any time. Importantly, the nurse did not ask him to recount additional details of what happened in his past. Next, the nurse verified his location and contact information and explained why obtaining this information was necessary. Next, she asked his consent to proceed with the visit, reminding him that the visit can end at any point if he feels uncomfortable. After finishing this initial discussion, the nurse told him that his primary care physician (PCP) would join the visit and address his concerns with his leg.
S was happy to see his PCP despite his hesitations about video care. The PCP noticed that he seemed anxious and was avoiding talking about the rash. Knowing that he was anxious about this VVC visit, the PCP was careful to look directly at the camera to make eye contact and to be sure her face was well lit and not in shadows. She gave him some time to acclimate to the virtual environment and thanked him for joining the visit. Knowing that he was a combat veteran, she warned him that there have been sudden, loud construction noises outside her window. Although the PCP was pressed for time, she was aware that S may have had a previous difficult experience around images of his body or even combat-related trauma. She gently brought up the rash and asked for permission to examine it, avoiding commands or personalizing language such as “show me your leg” or “take off your pants for me.”36After some hesitation, the patient revealed his leg that appeared to have multiple excoriations and old scars from picking. After the examination, the PCP waited until the patient’s leg was fully covered before beginning a discussion of the care plan. Together they collaboratively reviewed treatments that would soothe the skin. They decided to virtually consult a social worker to obtain emergency economic assistance and to speak with the patient’s care team psychologist to reduce some of the anxiety that may be leading to his leg scratching.