Reducing COPD Readmission Rates: Using a COPD Care Service During Care Transitions
A chronic obstructive pulmonary disease care service improves timely access to follow-up care and patient education at the time of transition from hospital to home.
Edward Portillo is a Clinical Pharmacist Specialist, Andrew Wilcox is Chief of Pharmacy Services, Ellina Seckel is Acting Chief of Primary Care and Associate Chief of Ambulatory and Specialty Care, Amanda Margolis is a Clinical Pharmacist Specialist, Jean Montgomery is a Physician in Primary Care, Prakash Balasubramanian i s a Hospitalist, Geri Abshire is the Northern Tier Clinic and Nurse Manager-Primary Care, Jim Lewis is Chief of Respiratory Therapy, Christopher Hildebrand is the Associate Chief of Staff for Education and Ambulatory Care, Sameer Mathur is Associate Professor in the Division of Allergy, Pulmonary and Critical Care Medicine, Alan Bridges is Chief of Staff, and Sujani Kakumanu is Chief of Allergy, all at the William S. Middleton Memorial Veterans Affairs Hospital in Madison, Wisconsin. Edward Portillo and Amanda Margolis are Clinical Assistant Professors at the University of Wisconsin-Madison School of Pharmacy. Christopher Hildebrand and Alan Bridges are Clinical Professors in the Department of Medicine, and Sameer Mathur is an Associate Professor at the University of Wisconsin-Madison School of Medicine and Public Health.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Methods
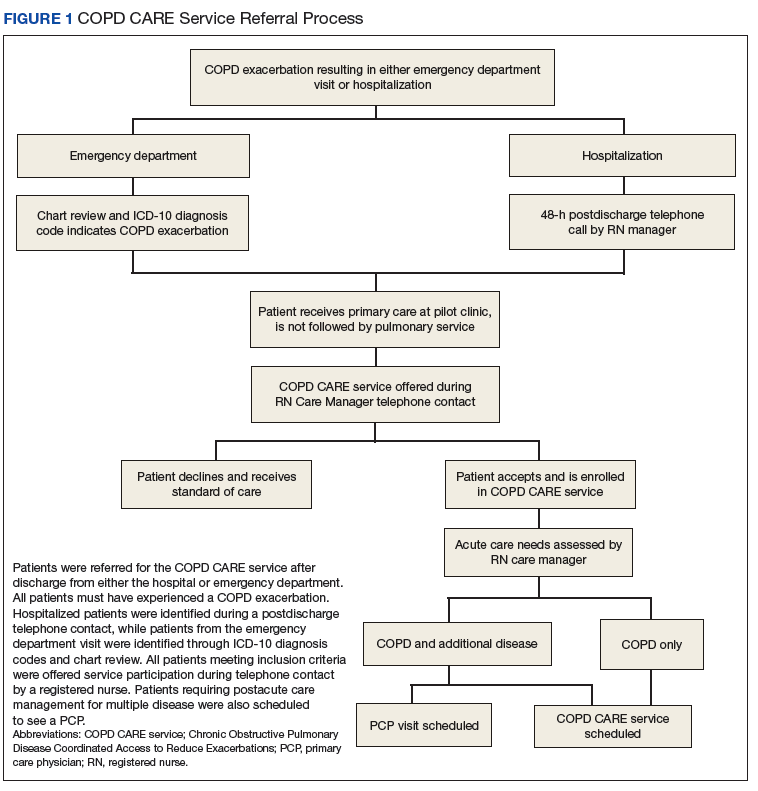
The COPD CARE service was implemented on October 1, 2015, and evaluated through March 1, 2016 (Figure 1). All veterans receiving primary care through the pilot clinic site with a hospital admission or ED visit for COPD exacerbation were offered this intervention.
Patients were identified by discharge visit ICD-10 codes specific for COPD. The clinic nurse care manager spoke with patients on the phone and offered the COPD CARE service.
Patient Eligibility and Recruitment
Patients were excluded from the service if COPD or COPD-related diagnoses were not listed in their electronic health record (EHR) problem list. Patients who had previously received components of the intervention through consultation with specialty services were excluded. If a patient declined the service, they received the standard of care. This project was undertaken for programmatic evaluation and qualified for quality improvement (QI) exemption; as such an internal review board approval was not required.
Intervention
Participants enrolled in the COPD CARE service were scheduled for an interprofessional postdischarge follow-up visit with a pharmacist and nurse at the pilot outpatient clinic site, and this visit was termed the COPD CARE health visit. Participants ideally were seen within 30 days of discharge. The goal was to improve access to care while preventing a 30-day readmission. Within this 30-day window, the target follow-up period was 2 to 3 weeks postdischarge for the face-to-face visit. Patients who required postdischarge care for additional medical conditions received a clinic appointment with their PCP on the same day as their COPD CARE health visit. The COPD CARE health visit focused on 3 objectives: (1) COPD disease management and referrals; (2) COPD plan development; and (3) inhaler technique review and teaching.20,21
COPD Monitoring
During the 45-minute COPD CARE health visit, the pharmacist provided extensive disease management based on the GOLD guideline recommendation.22 In addition, the pharmacist administered the COPD Assessment Test (CAT) and reviewed patient COPD exacerbation history to guide prescribing.22 The patient and pharmacist also reviewed previous spirometry results if obtained within the past 2 years. COPD triggers and symptoms were assessed along with opportunities for therapeutic and lifestyle modifications.
Plan Development
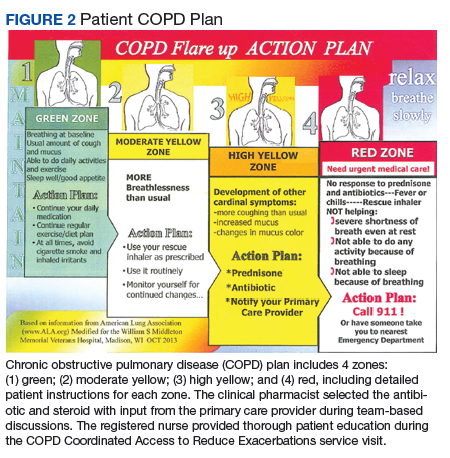
Patients in the COPD CARE service also were given a COPD plan to improve health outcomes. (Figure 2). The plan included patient instructions to initiate steroid and antibiotic therapy if the patient experienced symptoms of increased cough, mucus production, and purulence, thereby reaching the high-yellow zone.
The pharmacist prescribed the antibiotic and steroid therapy for the COPD plan within the PACT model and consulted the PCP to ensure effective, team-based decision making. The RN educated the patient on the plan with specific emphasis on how to use the plan to self-manage COPD symptoms. Patients were instructed to contact the clinic before starting plan medications so that a thorough assessment of symptoms could be performed. Patients who were noted to have decompensated COPD or with worsening symptoms were triaged to urgent medical care or to urgent appointments with the PCP.