Dr. Wrobel is a clinical associate professor of internal medicine at the University of Michigan Medical School in Ann Arbor. Dr. Kirsh is an associate professor and Dr. Robbins is a clinical assistant professor at Case Western Reserve University School of Medicine in Cleveland, Ohio. Dr. Pogach is a professor of preventative medicine and community health at Rutgers University-New Jersey Medical School in Newark. Dr. Robbins is a podiatrist and Dr. Kirsh is a physician, both at the Louis Stokes Cleveland VAMC in Ohio. Dr. Pogach is a physician at the VA New Jersey Health Care System in East Orange, New Jersey.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
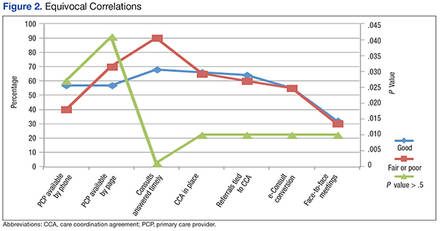
Figure 2 describes the equivocal correlations that were found between fair or poor self-reported centers and high-functioning PACT/Podiatry services with:
Presence of a signed CCA.
Multiple positive or negative characteristics.
Referrals tied to the CCA.
Provision to convert to an e-consult.
Face-to-face meetings to review the CCA.
Discussion
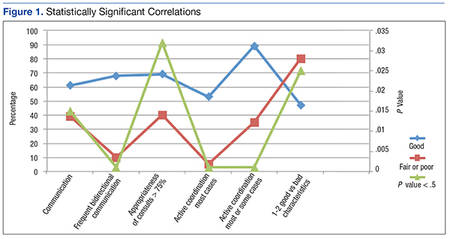
The key to high-functioning PACT/Podiatry teams rests with the quality of the communication between providers. Without this basic tenet, CCAs cannot be effective.
This tenet supports the authors’ prior work that found programming coordination was associated with lower rates of lower extremity amputations in patients with diabetes.8 Programming coordination consists of electronic medical records, policies, reminders, protocols, and educational seminars.8 In the present study, it seemed that the appropriateness of referrals were more important than having care coordination agreements.
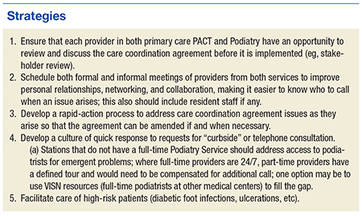
This concept also is supported in the authors’ prior work of developing a microsystem of foot care: Appropriateness of referrals was a “must do” associated with lower rates of major amputation.9 Developing good interdisciplinary communication requires the support of leadership, at least yearly face-to-face meetings between providers, buy-in for the components of the CCA, and a sustained relationship of patient-centered cooperation.
Conclusion
Self-reporting high-functioning PACT/Podiatry teams depend more on the relationships between providers, the ease of bidirectional communication and coordination of care, and a seemless consult and less on the formal care coordination documents and e-consults that reduce the direct exchanges between providers.
Effective communication that is responsive to dynamic changes will outperform dogmatic and static policy documents.