An ECHO-Based Program to Provide Geriatric Specialty Care Consultation and Education





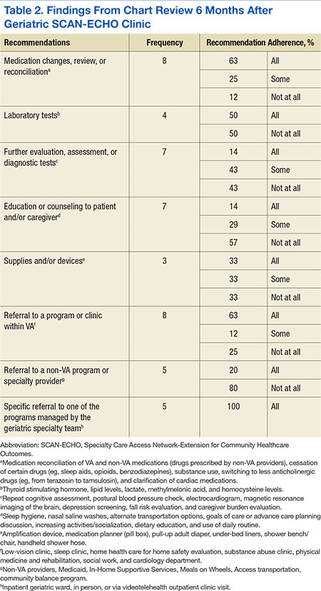
Table 2 lists the frequency and adherence to recommendations. If the recommendation was discussed but refused by the patient, it was still noted as completed. Several recommendations might have been presented; thus, adherence to recommendations was categorized as “all,” “some,” or “not at all” adherent. Because the referrals involved complex cases, most cases were referred to other clinical programs managed by the geriatric specialty team for further evaluation and management.
Discussion
Although the Geriatric SCAN-ECHO sessions were well received, the impact of the program was limited by the lack of consults and PACT team involvement. Impact was markedly improved once the focus of the sessions changed from case studies to specific clinical tool administration/practice change. Leadership support and coordination to provide protected team learning time was essential. Incentives to participate might include making geriatric quality indicators part of performance measures to improve practice and quality of care. Although the VA monitors several frail elderly measures that are a reflection of quality geriatric care, it is up to each VISN to determine its performance measures (Kenneth Shay, e-mail communication, February 12, 2013).
The most frequently followed recommendation was referral to a program managed by the geriatric specialty team. Full compliance with this recommendation may be due to the ease of placing a single consult and the interaction between the SCAN-ECHO team and the geriatric specialty services staff. The next most commonly followed recommendations were for medication changes/review and referral to a different program or clinic (not inpatient or outpatient geriatric specialty programs). Because completion of medication reconciliation reminders are tied to pay incentives for VA physicians, this may explain why it was fulfilled at a higher rates compared with other recommendations, suggesting that bonus incentives could boost participation.
The least frequently completed recommendations were referrals to non-VA programs or specialty providers. This may be a reflection of poor communication with non-VA providers and/or documentation of such communications and lack of the availability of the programs near the patient’s residence. Developing remote site referral guides might improve this communication.
Another type of recommendation that was partially or not at all followed was for further evaluation, assessment, or diagnostic tests of specific problems identified by the Geriatric SCAN-ECHO team. This may be due to lack of easy access to specific diagnostic tests in outpatient clinics or lack of staff knowledge and skills on doing geriatric-specific evaluations. The chart reviewer also noted that even when the PCP did the evaluations, the quality was below standard; for example, for depression screening, the chart noted that the patient was asked about having depression; however, no specific tool was used to aid in the diagnosis. Further specificity regarding geriatric syndrome evaluations and increasing staff knowledge of common tools to aid in diagnosis and evaluation are needed.
In 2 of the 8 cases reviewed, the Geriatric SCAN-ECHO program recommended that specific family members needed to be involved in the care of the patient. Unfortunately, most often family members only were used as a means of communication or for coordination of care with the PACT teams (eg, scheduling appointments). Changes needed to provide quality care for geriatric veterans are to include family members, use a fully-realized PACT approach, and have nurses “practice to the full extent of their education and training,” as recommended by the Institute of Medicine.9
Limitations
This article reported on the experience of a geriatric team that implemented an interdisciplinary telehealth-based consultation program. Facilitators and barriers to program execution may be limited to the local site and VA. The survey following the session was developed by the VA SCAN-ECHO program and was not specific to this local program. Limitations of the chart review include a short follow-up of only 6 months after the program. Many of the behavioral changes or educational recommendations might have been discussed but were not documented. Also services done by non-VA providers might not have been documented and, therefore, would not have been included in this chart review.
Conclusions
The geriatric team decided to discontinue the Geriatric SCAN-ECHO program. The key metric for program success was number of cases reviewed. Only 1 to 2 cases were reviewed every other month. Participation in the program markedly increased when the specific learning needs of PACT teams were addressed; however, most cases were referred to GRECC due to the case complexity and were not appropriate for the SCAN-ECHO format. The chart review, patient and caregiver contact, and presentation preparation required the program staff to invest a significant amount time. It took 3 to 4 hours for the staff to prepare for each case. Furthermore, adherence to recommendations was also poor.