Complementary and Alternative Medicine for Chronic Musculoskeletal Pain





Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
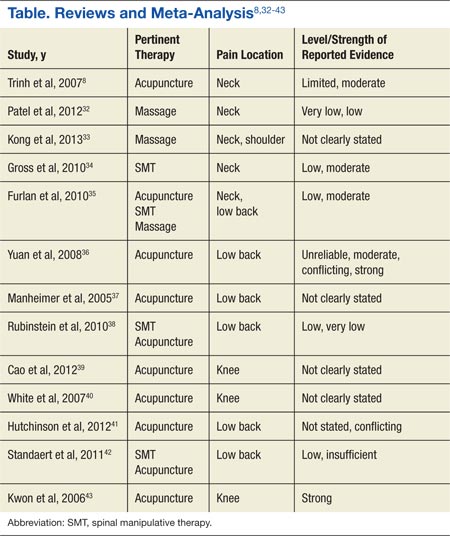
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46