How well do physician and patient visit priorities align?






This study found that there is alignment between a patient’s reason for a visit and the physician’s main concern 69% of the time. Less than fully aligned priorities were associated with insurance status and the number of problems addressed.
Data analysis
We computed descriptive statistics and performed bivariate tests of association between physician-patient alignment of priorities and patient/visit characteristics, using chi-square statistics for categorical variables and analysis of variance (ANOVA) for continuous variables. We used logistic regression analysis to identify characteristics independently associated with either partially aligned or totally unaligned visit priorities, vs fully aligned priorities.
To better understand the unaligned cases, the study team examined all of the data cards identified as either only partially aligned or totally unaligned and categorized the nature of the disparate prioritization in each case. Study team members (PT, AW, MR, and PDG) individually reviewed and sorted the cards into similar observed patterns and wrote brief descriptions of those patterns. The group refined the preliminary descriptions of the overarching patterns and selected several cases to represent the patterns.
RESULTS
Quantitative findings
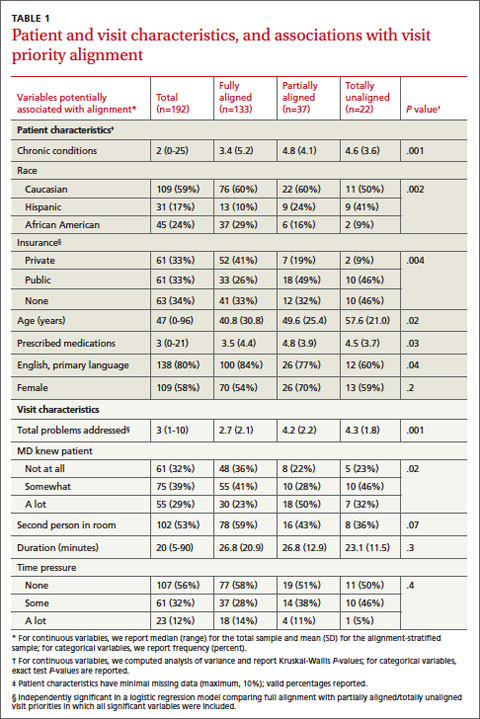
We collected data on 192 patients (TABLE 1). Median patient age was 47. Median number of prescription medications and chronic medical conditions were 3 and 2, respectively. Most patients (80%) primarily spoke English, 58% were female, and 59% were Caucasian. Insurance status was equally distributed among patients: 33% held private insurance, 33% had public insurance, and 34% were uninsured.
The majority of cases showed physician- patient priorities that were fully aligned (69%); only 12% were totally unaligned. TABLE 1 shows the associations between level of alignment and patient and visit characteristics. Patients whose expressed reason for their visit was less than fully aligned with their physicians’ primary concern were more likely to be older, with more chronic conditions, of Hispanic ethnicity, and either publicly insured or uninsured. Patients with some degree of unaligned concerns also tended to have greater numbers of prescribed medications and had a primary language other than English. Unaligned visit priorities were also observed more often when greater numbers of problems were addressed during the visit. Patients familiar to the physician were also more likely to express a reason for their visit that differed in some way from the primary concern of their family physician.
Multivariable logistic regression analyses showed that having more problems addressed during a visit and being publicly insured or uninsured (compared with having private insurance) were each independently associated with less than fully aligned visit priorities (indicated by § in TABLE 1).
Qualitative findings
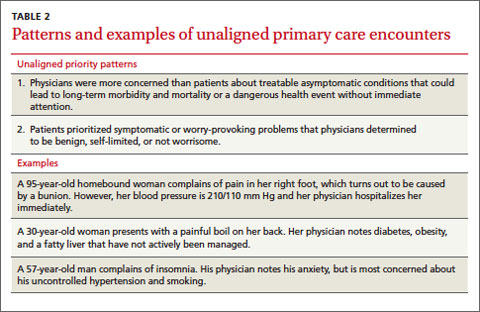
Cases classified as partially or totally unaligned showed 2 main patterns that reflect differences in the ways that patients and physicians prioritize problems. First, when physician priorities were unaligned with the patient’s stated reason for a visit, physicians typically focused on treatable, asymptomatic conditions that could lead to long-term morbidity and mortality or, absent immediate attention, to a dangerous event. Examples include chronic disease management (eg, hypertension, diabetes, asthma) and disease prevention (eg, smoking cessation, cholesterol level monitoring, cardiac disease risk reduction). Second, in those visits that were unaligned, patients tended to show more initial concern about symptomatic problems (eg, skin rash, upper respiratory infection) that would likely resolve with minimal or no medical intervention. Most of these conditions were determined by the physician to be benign, self-limited, or not worrisome (TABLE 2).
DISCUSSION
This study examined the alignment between a patient’s stated reason for a visit and the physician’s main concern. Physician-patient alignment was common, with 69% of visits showing full alignment between the patient’s reason for the visit and the physician’s main concern. While this rate is higher than that seen in prior studies,5 our method for data collection uniquely reflected how information actually is elicited and received during outpatient encounters, which likely yielded more accurate results. Also, in contrast to past approaches, our study equated patients’ symptoms to the underlying diagnosis for purposes of determining alignment.
Similar to previous studies, alignment between patient and physician concerns was less likely when the number of items addressed during the visit increased.5,6 Interestingly, physician-perceived time pressure during the visit and lack of an established patient-physician relationship were not observed to influence alignment. When time is limited, physicians may choose to prioritize the patient’s verbalized concern to avoid more complex negotiations about the agenda. In addition, during an encounter with an unfamiliar patient, prevention and chronic illness care may be deferred until the relationship becomes established.15-18
Patient insurance status was also observed to influence alignment. This finding could reflect socioeconomic or access issues among uninsured or publicly-insured patients that contribute to more complex visits.19-21 To shed further light on this finding, further research is needed that includes indicators of education or income and that separately examines Medicaid vs Medicare enrollees.