Overweight youth: Changing behaviors that are barriers to health






Practical advice for dealing with the family, the child, and socioeconomic environment.
Physical activity concepts are also often misunderstood by patients; for example, “screen time,” moderate intensity, cardiovascular fitness, and low impact. Using nutrition and activity terminology with patients does not guarantee good communication or goal achievement. Information and awareness, as well as myths and misinformation, were found to be barriers to weight improvement.22
Sociocultural barriers: A “fast food” culture and ever-present bias
Multiple studies have cited increased consumption of high energy/low cost foods including carbohydrates,23,24 fats, and sugars23,25 as a cause of child obesity. Many foods thought to be central to a healthy diet are perceived by some caregivers as too costly.9 The good taste, convenient preparation, and lower cost of foods with refined grains and added sugars and fats increase their popularity.26,27
Some neighborhood environments limit access to fruits and vegetables,28 resulting in increased rates of obesity. Restaurants, including the “fast food” kind, often serve large portions of unhealthy foods and thereby promote the ingestion of portions that are, literally, out of proportion to reason.29 Nutrient-dense lean meats, fish, and fruits and vegetables cost more per serving and do not satiate appetites as readily.
Unsafe neighborhoods cause significant anxiety in inner city parents and children30 and may discourage physical activity, thus increasing risk of overweight.31 In a study involving 20 large US cities, mothers’ perceptions of neighborhood safety related to their children’s television viewing time,32 and television viewing time has been shown to have a negative relationship to increased body mass index (BMI) in youth.33-35
Obese children may avoid physical activities that involve peers. Peers exert increasing influence on children and adolescents and ostracize those who are different. Bell et al showed that young children were less willing to engage an obese peer in physical activities,36 and overweight and obese children are more likely to be the victims of bullying as well as more likely to be the perpetrators of bullying than are normal weight peers.37
Although rates of childhood obesity among the general population are alarmingly high, they are higher still in ethnic minority and low-income communities.38 Low-income and minority children watch more television than white, non-poor children do. Neighborhoods where low-income and minority children live typically have more fast food restaurants and fewer vendors of healthful foods than do wealthier or predominantly white neighborhoods. Obstacles cited by Kumanyika38 are unsafe streets, dilapidated parks, and lack of facilities. In Hispanic youth, barriers in the school system include lack of facilities, equipment, and trained staff for physical education.39 Hispanic children are more sedentary than are white children40 and resultantly overweight.41
Enlist other caregivers to strengthen a treatment plan
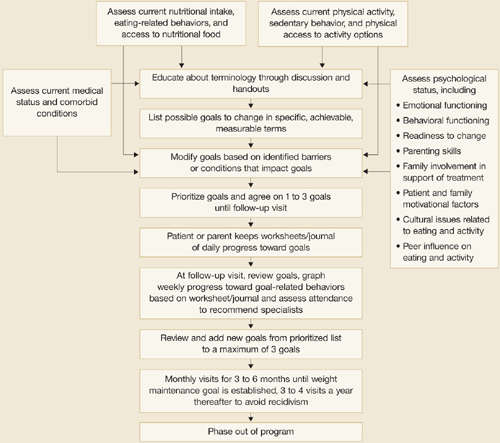
We promote a multidisciplinary approach—the short- and long-term benefits of which are supported by data59—to treating overweight youth: parental involvement, nutrition education, physical activity education, and behavior modification.42 Coordination among the healthcare professionals is important to avoid giving mixed messages to patients and to learn what each discipline uniquely discovers about barriers and ways to surmount them. Combining perspectives and information should lead to a stronger treatment plan (FIGURE) and greater treatment success. Online resources like the USDA’s MyPyramid.gov, are available to clinicians who do not have access to multidisciplinary clinic facilities.
Parents’ attitudes influence the child
Assess the family’s level of concern and willingness to participate in a treatment plan.44-46 Parents’ involvement is critical, especially given that parental concern about weight is a predictor of change in total fat mass over time, at least in Caucasian children.14 Only when parents see a child’s weight as a health problem are they likely to be motivated toward changing.43
Research suggests that the parents’ attitude toward physical activity affects a child’s attitude toward physical activity.19,47 In fact, parent changes in BMI have been found to predict child changes in BMI for overweight youth.48
Clinicians need to inform and engage family members in the assessment and behavioral change processes, uncover erroneous belief systems, identify family dynamics that may affect treatment, and assess parenting skills. For instance, feeding children every time they say they are hungry might not be in their best interest, especially if the food is used to satiate or modify emotions and behaviors. Parents need to understand how their roles in addressing nutrition and physical activity change as their children move through different developmental periods,49 suggesting a flexible parenting style that evolves as the child ages.
One method to determine the parental choices and behavior is to ask parents to keep a record of what the child eats and in what portion size. How much and what kind of exercise does the child receive? Over time, patterns emerge that allow a clinician to formulate a treatment plan based on eating and physical activity modification.
FIGURE
Key steps in managing overweight in children and youths