Schizophrenia: Recognition and Management in the ED






History
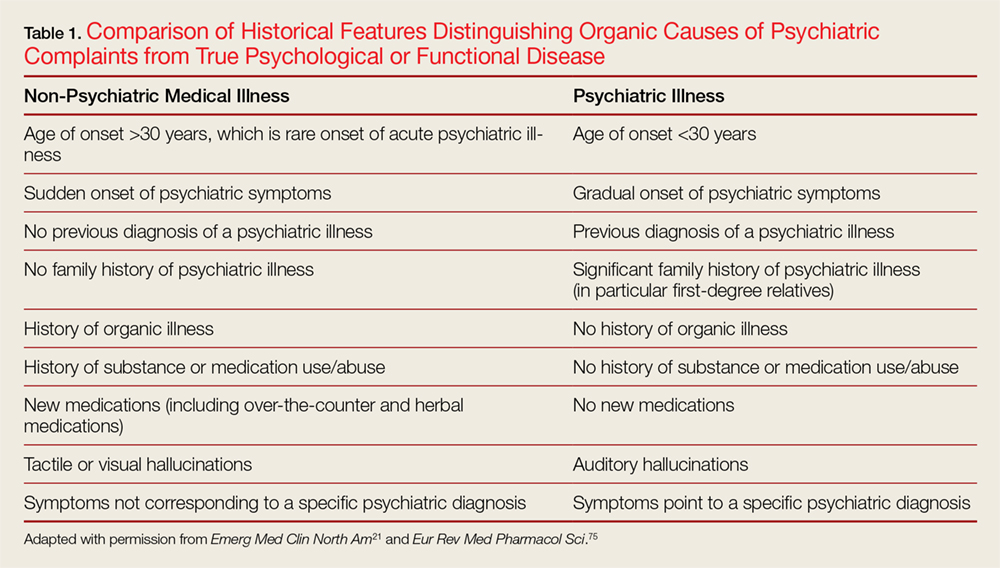
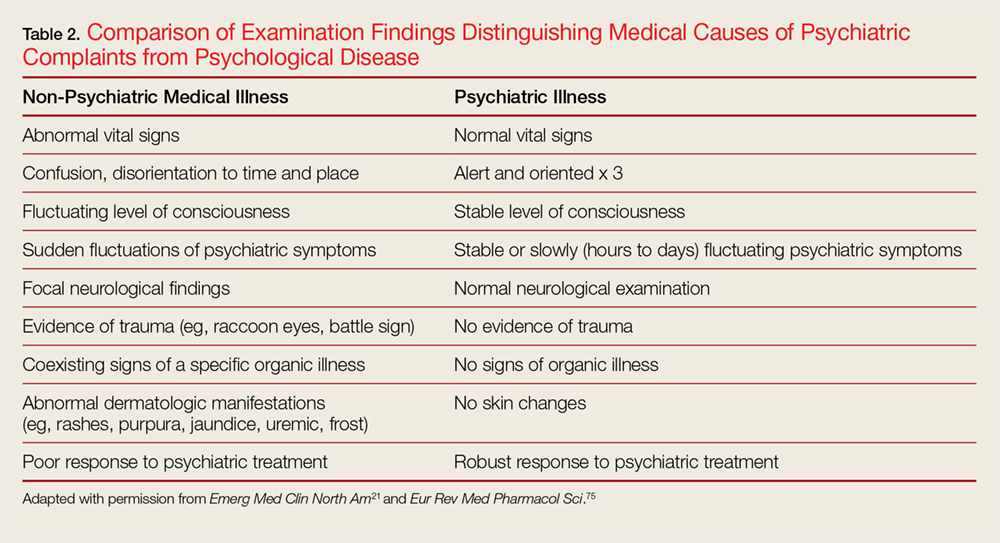
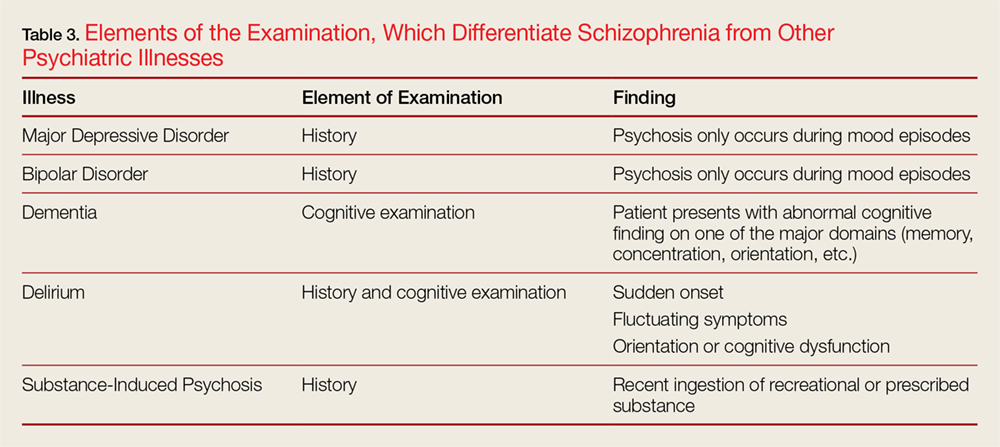
The history should focus on age of onset; prior history of psychiatric symptoms; history of medical illness and use or abuse of illicit substances, as well as medications; the stability of psychotic symptoms; and if hallucinations are present, whether they are auditory or visual in nature.10 Table 1 highlights the differences between a patient presenting with a psychiatric complaint and the psychotic symptoms secondary to a medical illness. Table 2 provides salient differences between the examination of a patient with psychosis due to a psychiatric illness or another medical condition. Additionally, Table 3 lists various features, which differentiates schizophrenia from other psychiatric illnesses.
Additionally, patients with schizophrenia can become just as physically ill as anyone else; however, they may have difficulty expressing their specific physical complaints. Furthermore, patients with schizophrenia have a pronounced incidence of early death compared to the general population.11 Therefore, performing a simple physical examination and paying attention to vital signs can rule out or detect a great deal of organic pathology.12Once a diagnosis of schizophrenia is made, the next priority is to determine whether the patient is a threat to themselves or others and whether this threat is imminent or not. Statements of suicidal or homicidal ideation, intent, and/or plan are the basic methods of screening for danger. However, physicians also need to screen for command auditory hallucinations, prior history of suicidal behavior, and violence. Finally, even in a patient with previously diagnosed schizophrenia, screening must also be done for substance intoxication and withdrawal.
Diagnostic Studies
The indications for diagnostic studies are influenced by whether the presentation is experiencing first break psychoses vs a presentation in a patient with known schizophrenia. In the former case there is a greater need for laboratory and other diagnostic tests. In the latter case minimal testing will likely be necessary. Patients with new onset psychiatric symptoms generally need extensive laboratory and radiographic evaluations, including a computed tomography scan of the head.9
For patients who have an established schizophrenia, extensive evidence supports that there is no need for testing and indeed more often results in false positives,11,13and selective testing based on findings in the history and physical examination is the correct strategy.11
Complicating the decision to obtain laboratory tests is the fact that many psychiatric facilities rely on referring hospitals to perform baseline testing, as they do not have the resources to perform the tests or to manage any identified abnormalities. Therefore, some tests are needed prior to transfer. In addition, at times, baseline laboratory tests are needed prior to starting antipsychotics.14
Additionally, some tests are unlikely to affect immediate disposition or treatment but may be useful to psychiatrists for long-term treatment planning.15 A common disagreement between psychiatrists and emergency providers is the urine toxicology screen or a blood alcohol level. Urine toxicology or a blood alcohol level does not usually affect initial treatment and disposition in the ED.11,16 However, it may be invalid if collected subsequent to a transfer from the ED, and can determine whether a patient requires specific substance use disorder treatment or not.16-18 Therefore, many psychiatric providers will request a urine toxicology screening or a blood alcohol level before accepting a transfer. Please note, urine toxicology screens only identify a small number of toxic ingestions. Therefore, a negative screen does not eliminate drug abuse or overdose.
Finally, in the case that a diagnostic examination is being done to satisfy a requirement for an institution to accept a patient or to assist in long-term treatment planning, disposition should not be delayed in order to wait for the result to return.11