Management of HIV/AIDS





With the advances in antiretroviral therapy and increased life expectancy of
patients with HIV infection, the emergency physician must also consider noninfectious pathologies in the differential diagnosis.
Primary HIV-related Disease—Wasting Syndrome. The AIDS wasting syndrome is defined as a weight loss of at least 10% body weight in the presence of diarrhea or chronic weakness and documented fever for at least 30 days that is not attributable to a concurrent condition other than HIV infection itself. Before HAART, the prevalence of wasting was estimated to be up to 37%.18 Some data suggest that the incidence of wasting syndrome is decreasing, however other studies indicate that wasting remains a significant complication, even in populations with widespread access to effective antiretroviral therapy.19 Treatment is multifaceted, including pharmacologic agents to stimulate appetite and muscle accrual, and is not primarily within the purview of the ED. However, the EP should be aware of the process, and it may be prudent to screen for electrolyte disturbances and other treatable complications.
Immune Reconstitution Inflammatory Syndrome
The reconstitution of the immune system after the initiation of HAART can sometimes exacerbate the symptoms of previously quiescent opportunistic infections, producing a paradoxical worsening of the HIV patient’s clinical status. This state is referred to as immune reconstitution inflammatory syndrome (IRIS). Although mycobacterial infections such as tuberculosis and M avium complex are the most common infections associated with IRIS, nearly all opportunistic pathogens have been reported as underlying triggers. IRIS generally manifests within the first 8 weeks after the initiation of antiretroviral therapy. Therapy is largely supportive, may include anti-inflammatories and steroids, and is aimed at the inciting opportunistic agent. Cessation of HAART is usually not required; however, in general these patients can become quite ill and often merit hospitalization.
Presentations Related to Complications of Antiretroviral Therapy
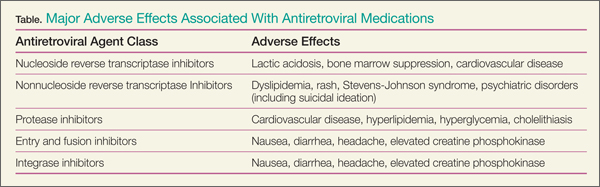
Hepatotoxicity and lactic acidosis are among the most common adverse reactions to antiretroviral therapy seen in the ED. All protease inhibitors are associated with hyperlipidemia, hyperglycemia, truncal obesity and an increased risk of atherosclerosis (Table). Multiple studies have shown that HIV infection and treatment with HAART increases an individual’s relative risk of acute MI. Patients receiving HAART should be considered to have an elevated risk of acute coronary syndromes, often at younger ages than the general population.20
Postexposure Prophylaxis
There are two broad categories of postexposure prophylaxis (PEP) against HIV: occupational exposures (eg, needle stick injuries, conjunctival splashes) and nonoccupational exposures (eg, IV drug users, patients presenting after a sexual assault or a “high-risk” sexual encounter). Vertical, or mother-to-child transmission, is not primarily managed within the purview of the ED and will not be discussed here.
Although the considerations, counseling, and guidelines of these two types of exposures are different, the basic principles of PEP are the same. The US Public Health Service (USPHS) updated guidelines21 from 2013 include the following recommendations:
1. Initiate antiretroviral therapy as soon as possible after exposure, ideally within 2 hours. If the source patient’s HIV status is not known or immediately available, administration of PEP should not be delayed. After 72 hours there is little data to support the use of PEP, and it is not routinely recommended except on a case-by-case basis.
2. A minimum three-drug regimen is recommended; although the most recent update to the USPHS guidelines for nonoccupational prophylaxis, made in 2005, suggest a two-drug regimen is sufficient, the majority of more recent national and regional guidelines recommend a three-drug regimen for both types of exposures.
3. The PEP should continue for 28 days.
4. Testing for other sexually-transmitted and blood-borne diseases such as hepatitis, syphilis, gonorrhea, and chlamydia should be considered. In women presenting after sexual assault, emergency contraception should be offered.
5. Potential side effects should be discussed, and prophylactic therapy, such as antiemetics, should be considered for those initiating PEP.
Assessing Risk After a Potential Exposure
Many factors affect the risk of acquiring HIV after a single exposure. A number of epidemiologic studies have calculated the risk of HIV seroconversion after a single needle-stick injury from HIV-contaminated blood at around 0.3%.22 A meta-analysis in 2006 included 22 studies on accidental percutaneous injury with risk ranging from 0% to 2.38%, and concluded that the pooled estimate per exposure is 0.23%.Due to source patient factors and the type of exposure, the actual risk for a particular occupational exposure may be substantially higher or lower.23
Despite the difficulties in assessing true risk to a particular individual after an exposure to HIV, pooled estimates are helpful in determining the cost-benefit analysis of PEP. According to the CDC, the risk of seroconversion after mucocutaneous exposure is thought to be 0.1%. There is considered to be no risk of HIV transmission where intact skin is exposed to HIV-infected blood. A case-control study in the late 1990s identified four factors that increased risk of transmission: deep injury, visible blood on the device causing injury, injury with a needle that had been placed in blood vessel, and advanced HIV-status of the source patient.24