
Acitretin-Induced Acral Hemorrhagic Lesions in Darier-White Disease





Darier-White disease (DD) is an autosomal-dominant inherited disease characterized by keratotic papules that are usually located in seborrheic areas. Systemic retinoids generally are first-line treatment in cases of diffuse DD. We report the case of an 84-year-old woman with a hypertrophic variant of DD with acral lesions. Oral retinoids (acitretin) were administered as a first treatment of DD, with good clinical results. After a few months, hemorrhagic vesicles developed on palmoplantar surfaces. Suspension of the therapy led to the disappearance of the cutaneous manifestations.
Practice Points
- The first-line treatment of Darier-White disease (DD) is oral retinoids.
- Numerous side effects of retinoids have been described. Clinicians should take these cutaneous manifestations into consideration in patients affected by DD.
Darier-White disease (DD), also known as keratosis follicularis, is a rare skin disease that is inherited in an autosomal-dominant fashion. It was first described by both Darier1 and White2 more than 120 years ago. The incidence is 1 to 9 per 100,000 individuals, and onset usually occurs between 8 and 15 years of age. Classic DD is characterized by malodorous, brown, keratotic, warty papules arising mainly in seborrheic areas; palmoplantar pits; and nail dystrophy with typical worsening in summer. Unilateral and segmental variants of DD rarely have been described.3,4
Few cases of hemorrhagic DD involving acral surfaces have been reported.5-8 Most patients develop hemorrhagic bullae at the onset of the disease together with the other characteristic features of DD. The disease also can be associated with salivary gland obstruction, renal and testicular agenesis, bone cysts, and neuropsychiatric disorders.9 Diagnosis is confirmed by hyperkeratosis, papillomatosis, acantholysis, dyskeratosis (corps ronds and grains), and small fissures above the basal layer in the epidermis (suprabasal clefts) noted on biopsy of papular lesions. Darier-White disease is caused by a malfunctioning sarcoplasmic/endoplasmic reticulum calcium pump, SERCA2, encoded by the ATP2A2 (ATPase, Ca++ transporting, cardiac muscle, slow twitch 2) gene, which transports calcium ions from the cytosol into the sarcoplasmic/endoplasmic reticulum, catalyzing the hydrolysis of adenosine triphosphate coupled with the transport of the calcium. Mutations in ATP2A2 have only been identified in up to 50% of reported DD patients.10
Treatment of localized DD usually includes emollients and topical retinoids, and systemic retinoids are recommended as the first-line treatment of diffuse DD.11 Many dermatologic side effects of systemic retinoids have been reported, including frequent dry lips and cheilitis.12 Other skin manifestations include scaling of the palms and soles, excoriations and erosions, alopecia, pruritus, nail fragility, and skin atrophy or fragility. Additionally, common nondermatologic side effects include hepatotoxicity, epistaxis, ophthalmologic effects (eg, loss of eyebrows or eyelashes, redness/swelling of the eyelid, redness of the eyes, sensitivity of the eyes to light, decreased night vision) pancreatitis, bipedal edema, and skeletal alterations.13-15 We report the case of a patient with DD who developed hemorrhagic macules and vesicles in response to the administration of oral retinoids.
Case Report
An 84-year-old woman was admitted to our hospital for treatment of hyperkeratotic papules and plaques on the face, back, groin, submammary folds, and dorsum of the hands and feet that had been present since childhood and typically worsened during the summer. She previously had refused treatment and reported a poor social life due to the cutaneous manifestations of her disease.
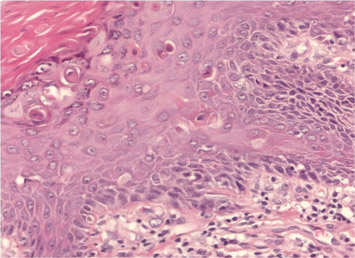
Biopsy of a histologic specimen taken from a palmar pit revealed hyperkeratosis, loss of cohesion between suprabasal epidermal cells (acantholysis), and dyskeratotic cells (corps ronds and grains)(Figure 1). On the basis of both clinical and histologic findings, a diagnosis of DD was made. Genetic analysis did not reveal any mutations in the ATP2A2 gene, and a reduced epidermal expression of SERCA2b was demonstrated by immunochemistry.16 Treatment with the oral retinoid acitretin (25 mg daily) for 4 months led to almost complete resolution of the lesions. After 4 months, treatment was reduced to a maintenance dose of 12.5 mg once daily.
The patient returned monthly for follow-up to undergo clinical examination and routine laboratory tests (ie, complete blood cell counts, electrolyte panel, renal and hepatic tests, serum lipid levels, cholesterol level). After beginning the maintenance dose, she returned for follow-up every 2 months.
On follow-up 3 months after beginning the maintenance dose, the patient reported the onset of red and black punctiform macules and vesicles with jagged borders located on the palmoplantar surfaces and dorsal aspect of the fingers on both hands. Lesions were either isolated or confluent. The patient did not report pain or itching, though the skin was severely xerotic, especially on the hands and feet (Figures 2A and 2B). The patient reported no local trauma associated with the lesions, and blood counts and coagulation tests were within reference range. It also was noted that the cutaneous manifestations of DD showed a striking improvement. Histologic analysis of a skin biopsy taken from a hemorrhagic lesion on the palmar surface showed hyperkeratosis, acanthosis, papillomatosis, hypergranulosis, focal dyskeratosis, and hemorrhagic vesicles in the horny layer of the epidermis (Figure 3), leading to a diagnosis of DD.
After 12 months of therapy, the patient spontaneously stopped taking acitretin, and the hemorrhagic lesions spontaneously regressed within 2 weeks (Figures 2C and 2D). Unfortunately, the cutaneous manifestations of DD (eg, papular lesions) progressively reappeared in the previously reported sites. Based on this relapse, the patient was advised to restart treatment with acitretin (25 mg daily). In the follow-up visit 1 month after restarting acitretin, physical examination revealed the reappearance of hemorrhagic lesions on the palmoplantar surfaces and the dorsal aspect of the fingers.
