Dr. Shah is from the Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota. Dr. Dacso and Ms. Schupbach are from the Center for Dermatology and Cosmetic Laser Surgery, Plano, Texas. Dr. Elston is from the Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, Charleston.
The authors report no conflict of interest.
Correspondence: Dirk M. Elston, MD, Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, 135 Rutledge Ave, 11th Floor, MSC 578, Charleston, SC 29425 (elstond@musc.edu).
Primary sebaceous carcinoma also can mimic metastatic adenocarcinoma within the skin and is histologically similar to metastatic adenocarcinomas. The most distinguishing feature is sebaceous differentiation characterized by sebocytes, which have a vacuolated cytoplasm giving the nucleus a scalloped appearance, frequently with adjacent ductlike structures (Figure 5). Epidermotropism sometimes is present in sebaceous carcinomas but cannot be relied on as a distinguishing feature. Immunohistochemical analysis also is a helpful tool; these tumors typically are positive for p63 and podoplanin, distinguishing them from negative-staining metastatic adenocarcinomas.10,11
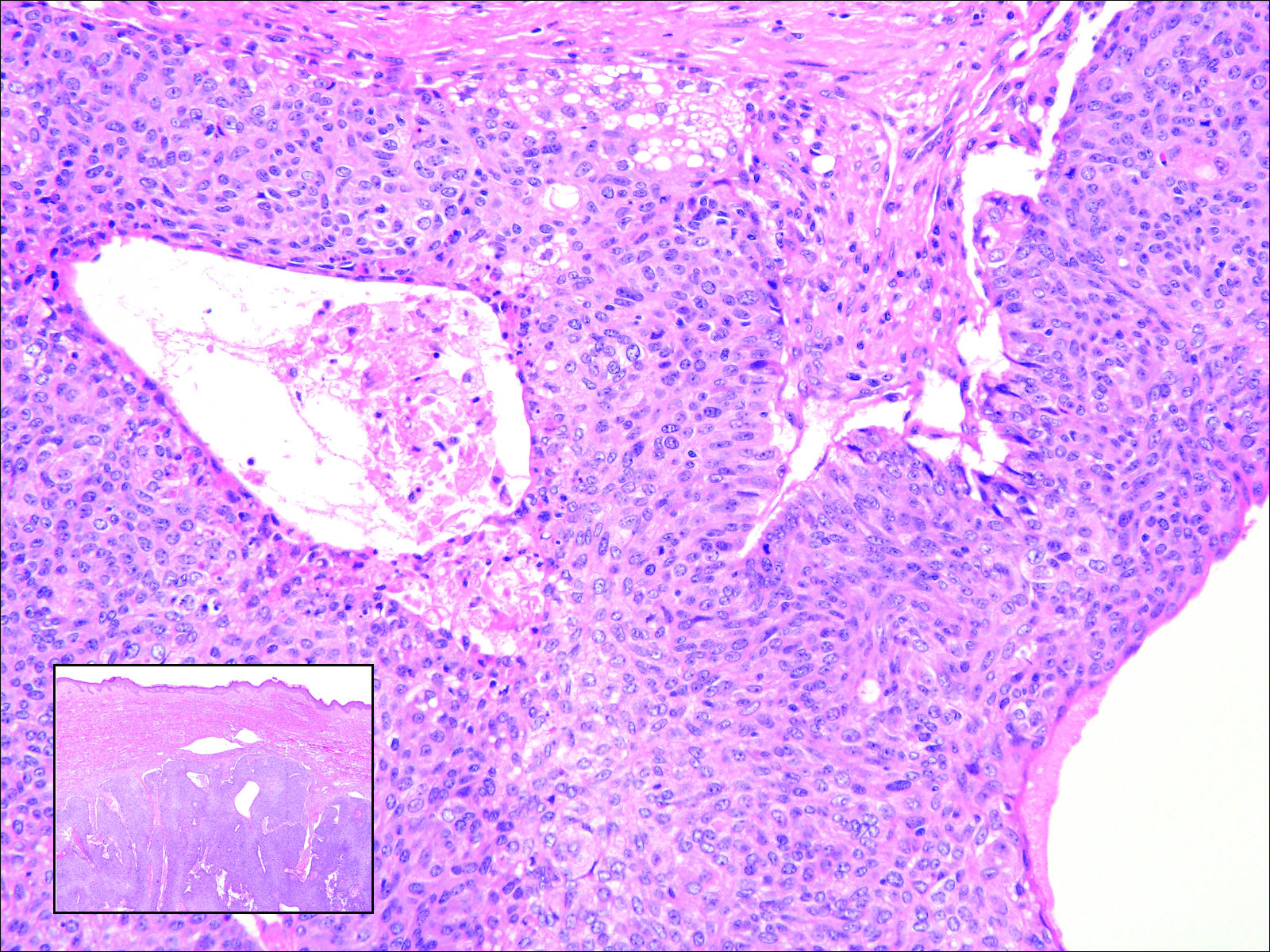
Figure 5. Within the dermis is a dense collection of atypical cells (inset [H&E, original magnification ×20]) with an unaffected overlying epidermis. At higher magnification, the atypical cells are elongated with abundant eosinophilic cytoplasm. Ductlike structures and vacuolated cytoplasm are characteristic of sebaceous carcinoma (H&E, original magnification ×400).
,false