Update in Hospital Medicine: Practical Lessons from the Literature





BACKGROUND: Hospital Medicine has a widening scope of practice. This article provides a summary of recent high-impact publications for busy clinicians who provide care to hospitalized adults.
METHODS: The authors reviewed articles published between March 2016 and March 2017 for the Update in Hospital Medicine presentations at the 2017 Society of Hospital Medicine and Society of General Internal Medicine annual meetings. Nine of the 20 articles presented were selected for this review based on the article quality and potential to influence practice.
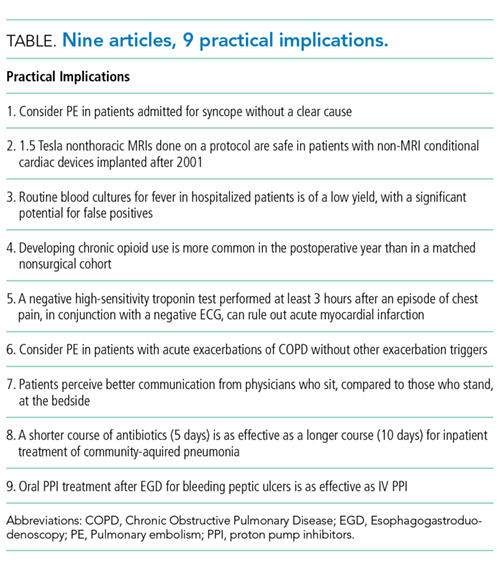
RESULTS: The key insights gained include: pulmonary embolism may be a more common cause of syncope and acute exacerbation of COPD than previously recognized; nonthoracic low-tesla MRI is safe following a specific protocol for patients with cardiac devices implanted after 2001; routine inpatient blood cultures for fever are of a low yield with a false positive rate similar to the true positive rate; chronic opioid use after surgery occurs more frequently than in the general population; high-sensitivity troponin and a negative ECG performed 3 hours after an episode of chest pain can rule out acute myocardial infarction; sitting at patients’ bedsides enhances patients’ perception of provider communication; 5 days of antibiotics for community-acquired pneumonia is equivalent to longer courses; oral proton pump inhibitors (PPI) are as effective as IV PPIs after an esophagogastroduodenoscopy (EGD) for the treatment of bleeding peptic ulcers.
CONCLUSIONS: Recent research provides insight into how we approach common medical problems in the care of hospitalized adults. These articles have the potential to change or confirm current practices.
© 2018 Society of Hospital Medicine
ESSENTIAL PUBLICATIONS
Prevalence of Pulmonary Embolism among Patients Hospitalized for Syncope. Prandoni P et al. New England Journal of Medicine, 2016;375(16):1524-31.1
Background
Pulmonary embolism (PE), a potentially fatal disease, is rarely considered as a likely cause of syncope. To determine the prevalence of PE among patients presenting with their first episode of syncope, the authors performed a systematic workup for pulmonary embolism in adult patients admitted for syncope at 11 hospitals in Italy.
Findings
Of the 2584 patients who presented to the emergency department (ED) with syncope during the study, 560 patients were admitted and met the inclusion criteria. A modified Wells Score was applied, and a D-dimer was measured on every hospitalized patient. Those with a high pretest probability, a Wells Score of 4.0 or higher, or a positive D-dimer underwent further testing for pulmonary embolism by a CT scan, a ventilation perfusion scan, or an autopsy. Ninety-seven of the 560 patients admitted to the hospital for syncope were found to have a PE (17%). One in
Cautions
Nearly 72% of the patients with common explanations for syncope, such as vasovagal, drug-induced, or volume depletion, were discharged from the ED and not included in the study. The authors focused on the prevalence of PE. The causation between PE and syncope is not clear in each of the patients. Of the patients’ diagnosis by a CT, only 67% of the PEs were found to be in a main pulmonary artery or lobar artery. The other 33% were segmental or subsegmental. Of those diagnosed by a ventilation perfusion scan, 50% of the patients had 25% or more of the area of both lungs involved. The other 50% involved less than 25% of the area of both lungs. Also, it is important to note that 75% of the patients admitted to the hospital in this study were 70 years of age or older.
Implications
After common diagnoses are ruled out, it is important to consider pulmonary embolism in patients hospitalized with syncope. Providers should calculate a Wells Score and measure a D-dimer to guide the decision making.
Assessing the Risks Associated with MRI in Patients with a Pacemaker or Defibrillator. Russo RJ et al. New England Journal of Medicine, 2017;376(8):755-64.2
Background
Magnetic resonance imaging (MRI) in patients with implantable cardiac devices is considered a safety risk due to the potential of cardiac lead heating and subsequent myocardial injury or alterations of the pacing properties. Although manufacturers have developed “MRI-conditional” devices designed to reduce these risks, still 2 million people in the United States and 6 million people worldwide have “non–MRI-conditional” devices. The authors evaluated the event rates in patients with “non-MRI-conditional” devices undergoing an MRI.