Safe Opioid Prescribing for Acute Noncancer Pain in Hospitalized Adults: A Systematic Review of Existing Guidelines





BACKGROUND: Pain is common among hospitalized patients. Inpatient prescribing of opioids is not without risk. Acute pain management guidelines could inform safe prescribing of opioids in the hospital and limit associated unintended consequences.
PURPOSE: To evaluate the quality and content of existing guidelines for acute, noncancer pain management.
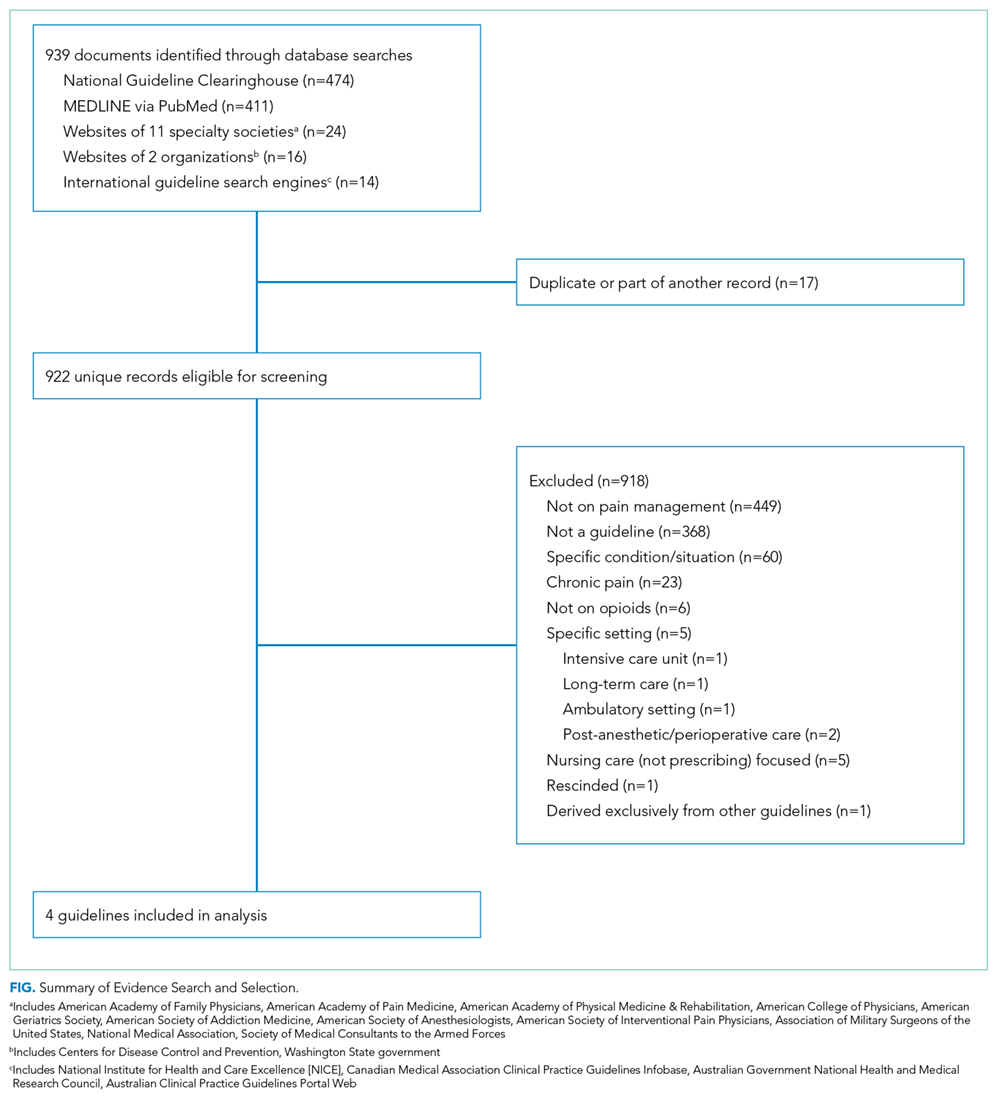
DATA SOURCES: The National Guideline Clearinghouse, MEDLINE via PubMed, websites of relevant specialty societies and other organizations, and selected international search engines.
STUDY SELECTION: Guidelines published between January 2010 and August 2017 addressing acute, noncancer pain management among adults were considered. Guidelines that focused on chronic pain, specific diseases, and the nonhospital setting were excluded.
DATA EXTRACTION: Quality was assessed using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument.
DATA SYNTHESIS: Four guidelines met the selection criteria. Most recommendations were based on expert consensus. The guidelines recommended restricting opioids to severe pain or pain that has not responded to nonopioid therapy, using the lowest effective dose of short-acting opioids for the shortest duration possible, and co-prescribing opioids with nonopioid analgesics. The guidelines generally recommended checking the prescription drug monitoring program when prescribing opioids, developing goals for patient recovery, and educating patients regarding the risks and side effects of opioid therapy. Additional recommendations included using an opioid-dose conversion guide, avoidance of co-administration of parenteral and oral opioids, and using caution when co-prescribing opioids with other central nervous system depressants.
CONCLUSIONS: Guidelines, based largely on expert opinion, recommend judicious prescribing of opioids for severe, acute pain. Future work should assess the implications of these recommendations on hospital-based pain management.
© 2018 Society of Hospital Medicine
Pain is prevalent among hospitalized patients, occurring in 52%-71% of patients in cross-sectional surveys.1-3 Opioid administration is also common, with more than half of nonsurgical patients in United States (US) hospitals receiving at least one dose of opioid during hospitalization.4 Studies have also begun to define the degree to which hospital prescribing contributes to long-term use. Among opioid-naïve patients admitted to the hospital, 15%-25% fill an opioid prescription in the week after hospital discharge,5,6 43% of such patients fill another opioid prescription 90 days postdischarge,6 and 15% meet the criteria for long-term use at one year.7 With about 37 million discharges from US hospitals each year,8 these estimates suggest that hospitalization contributes to initiation of long-term opioid use in millions of adults each year.
Additionally, studies in the emergency department and hospital settings demonstrate large variations in prescribing of opioids between providers and hospitals.4,9 Variation unrelated to patient characteristics highlights areas of clinical uncertainty and the corresponding need for prescribing standards and guidance. To our knowledge, there are no existing guidelines on safe prescribing of opioids in hospitalized patients, aside from guidelines specifically focused on the perioperative, palliative care, or end-of-life settings.
Thus, in the context of the current opioid epidemic, the Society of Hospital Medicine (SHM) sought to develop a consensus statement to assist clinicians practicing medicine in the inpatient setting in safe prescribing of opioids for acute, noncancer pain on the medical services. We define “safe” prescribing as proposed by Aronson: “a process that recommends a medicine appropriate to the patient’s condition and minimizes the risk of undue harm from it.”10 To inform development of the consensus statement, SHM convened a working group to systematically review existing guidelines on the more general management of acute pain. This article describes the methods and results of our systematic review of existing guidelines for managing acute pain. The Consensus Statement derived from these existing guidelines, applied to the hospital setting, appears in a companion article.
METHODS
Steps in the systematic review process included: 1) searching for relevant guidelines, 2) applying exclusion criteria, 3) assessing the quality of the guidelines, and 4) synthesizing guideline recommendations to identify issues potentially relevant to medical inpatients with acute pain. Details of the protocol for this systematic review were registered on PROSPERO and can be accessed at https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=71846.
Data Sources and Search Terms
Guideline Inclusion/Exclusion Criteria
We defined guidelines as statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harm of alternative care options, consistent with the National Academies’ definition.11 To be eligible, guidelines had to be published in English and include recommendations on prescribing opioids for acute, noncancer pain. We excluded guidelines focused on chronic pain or palliative care, guidelines derived entirely from another guideline, and guidelines published before 2010, since such guidelines may contain outdated information.12 Because we were interested in general principles regarding safe use of opioids for managing acute pain, we excluded guidelines that focused exclusively on specific disease processes (eg, cancer, low-back pain, and sickle cell anemia). As we were specifically interested in the management of acute pain in the hospital setting, we also excluded guidelines that focused exclusively on specific nonhospital settings of care (eg, outpatient care clinics and nursing homes). We included guidelines related to care in the emergency department (ED) given the hospital-based location of care and the high degree of similarity in scope of practice and patient population, as most hospitalized adults are admitted through the ED. Finally, we excluded guidelines focusing on management in the intensive care setting (including the post-anesthesia care unit) given the inherent differences in patient population and management options between the intensive and nonintensive care areas of the hospital.
