Integrated Fragility Hip Fracture Program: A Model for High Quality Care





BACKGROUND: Hip fractures are a significant cause of morbidity and mortality among elderly patients. Coordinated multidisciplinary care is required to optimize medical outcomes.
OBJECTIVE: To determine the effect of the implementation of standardized, evidence-based protocols on clinical outcomes and mortality in patients with fragility hip fractures.
INTERVENTIONS: A multidisciplinary group was convened to define best practices in fragility hip fracture care and implement a fragility hip fracture clinical protocol at Yale-New Haven Hospital. Clinical outcomes in 2015, prior to program initiation, were compared with 2018, after the program was well established.
MAIN OUTCOMES AND MEASURES: Measured outcomes included 30-day mortality, blood transfusion utilization, adverse effects of drugs, venous thromboembolic complications, sepsis, myocardial infarction, mechanical surgical fixation complications during the index admission, length of stay, 30-day readmission, unexpected return to the operating room (OR) and time to the OR.
RESULTS: The implementation of the Integrated Fragility Hip Fracture Program was associated with significant reductions in 30-day mortality from 8.0% in 2015 to 2.8% in 2018 (P = .001). Significant reductions were also seen in use of blood transfusions (46.6% to 28.1%; P < .001), adverse effects of drugs (4.0% to 0%; P < .001), length of stay (5.12 to 4.47 days; P = .004), unexpected return to the OR (5.1% to 0%; P < .001), and time to the OR <24 hours (41.8% to 55.0%, P = .001). CONCLUSIONS: An Integrated Fragility Hip Fracture Program using multidisciplinary care, physician and nursing engagement, evidence-based protocols, data tracking with feedback, and accountability can reduce mortality and improve clinical outcomes in patients with hip fractures.
© 2020 Society of Hospital Medicine
Hip fractures are a significant cause of morbidity and mortality among elderly patients. Patients with fragility hip fractures often carry multiple comorbid diagnoses with a significant risk of perioperative complications. After hip fracture, 30-day mortality has been reported as 3.3% to 17.2% with one-year mortality as high as 50%.1
Multidisciplinary care,2-5 surgery within 24 hours (h),6-12 use of regional peripheral nerve blocks,13-16 restrictive blood transfusion strategies,17,18 tranexamic acid (TXA) use,19 pharmacologic deep venous thrombosis (DVT) prophylaxis,20 surgical site infection prevention protocols,21 early mobilization,22 and nutritional optimization23-25 have been individually shown to improve outcomes in hip fracture patients.
Our program sought to define, standardize, and implement evidence-based best practices to improve clinical care and outcomes of patients with hip fractures. We convened a Center for Musculoskeletal Care (CMC) Hip Fracture Oversight Group that included surgeons and advanced practice providers from Orthopedics; physicians from Internal Medicine Hospitalist, Geriatrics, Emergency Medicine, and Anesthesia; and representatives from rehabilitation services, nursing, care management, pharmacy, and performance improvement. With clinical input from all involved services, we developed evidence-based protocols to standardize the care of patients with fragility hip fractures from the time of the patient’s evaluation in the emergency room to discharge and outpatient rehabilitation. The program was operationalized in February 2016.
This project was considered by the Yale University institutional review board (IRB) to be a quality improvement and, therefore, exempted from IRB approval.
MATERIALS AND METHODS
Yale-New Haven Hospital is composed of two main campuses. The York Street Campus (YSC) is the Level 1 Trauma Center. The St. Raphael’s Campus (SRC) houses the CMC nursing units for elective lower extremity arthroplasty and spine procedures. Prior to 2016, patients with hip fractures were cared for equally at both Yale-New Haven Hospital campuses. Patients were admitted to both medical and surgical services with no standardization of hip fracture care processes. Surgeons were assigned based on availability. Frequently, patients were added on to the operating room (OR) schedule and did not undergo surgery until off-hours and after a prolonged waiting period.
Medical comanagement of patients with fragility hip fractures at our institution predated the start of our CMC Integrated Fragility Hip Fracture Program (IFHFP). Comanagement was instituted in 2012 at YSC and in 2014 at SRC but without standardized protocols. The IFHFP began in February 2016 with the centralization of all patients with fragility hip fractures to the SRC at Yale-New Haven Hospital. Emergency medical services directed patients with suspected hip fractures to the designated campus. A dedicated hip fracture OR was allocated daily with a hip fracture surgeon assigned by a shared community and faculty surgeon call schedule. Patients were encouraged but not required to accept care from the on-call hip fracture surgical attending. Anesthesia was notified of the arrival of a patient with a hip fracture in the emergency department, and if the patient consented and qualified, a single-shot femoral nerve block was performed. Patients were screened for nasal staphylococcal colonization and treated with povidone-iodine nasal decolonization, chlorhexidine wash, and antibiotics determined by staphylococcal status and type of surgical procedure planned. Preoperative and postoperative order sets were implemented that dictated the care processes as outlined in Table 1. Surgeons determined the choice of operative intervention as per usual; this included internal fixation and partial or total hip replacement. Detailed medical and surgical protocols are included in Appendix A.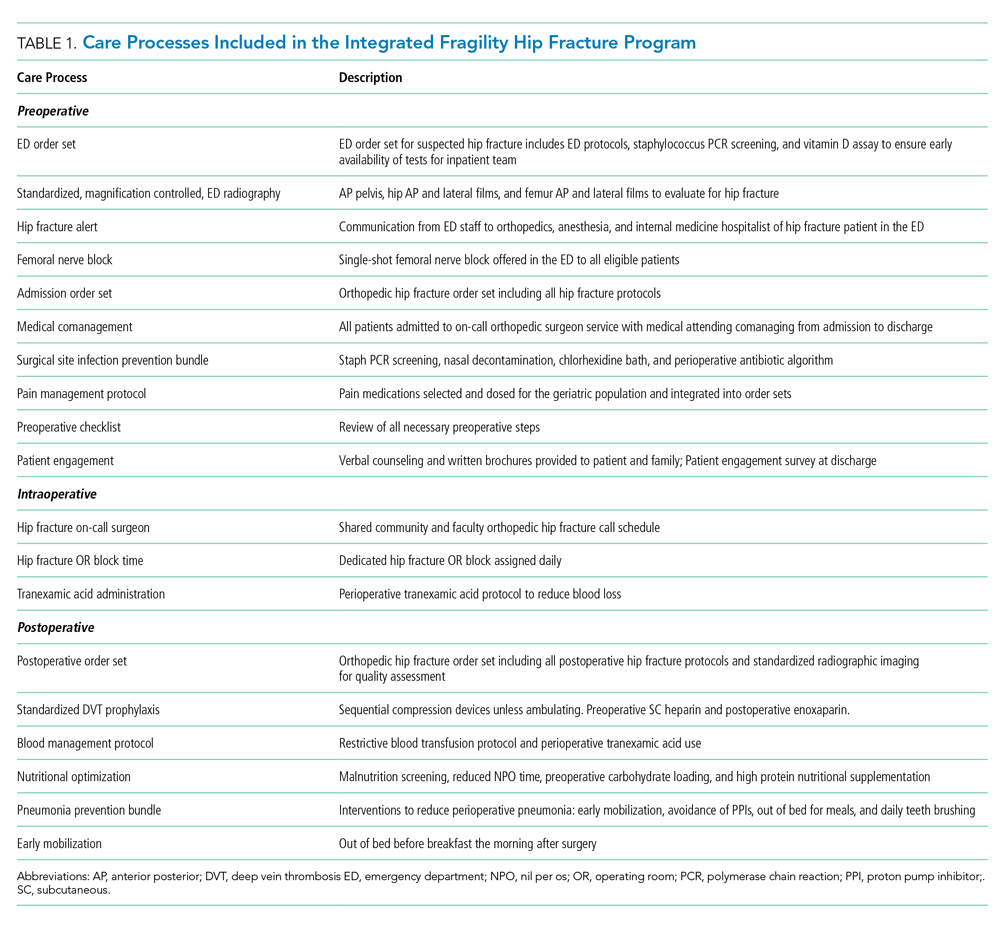
Since the initiation of the IFHFP on February 1, 2016, the program has continued to advance with our experience. We used the year preceding the start of the program as our baseline year (January 1, 2015, through December 31, 2015). The following years, 2016 and 2017, were a transition time during which our protocols were implemented. The intervention year was defined as January 1, 2018, through December 31, 2018. The outcomes during the intervention year were compared with the baseline year. It is important to note that our program has been in continuous evolution, including during the intervention year, with protocols created and refined as we gain experience.
Outcomes include 30-day mortality, transfusions, adverse effects of drugs, venous thromboembolic complications, sepsis, myocardial infarction, mechanical surgical fixation complications, length of stay, 30-day readmission rate, unexpected return to the OR, and time to operative intervention. Definitions of the outcome variables are reviewed in Appendix B.
