The diagnosis: Spontaneous gallbladder perforation
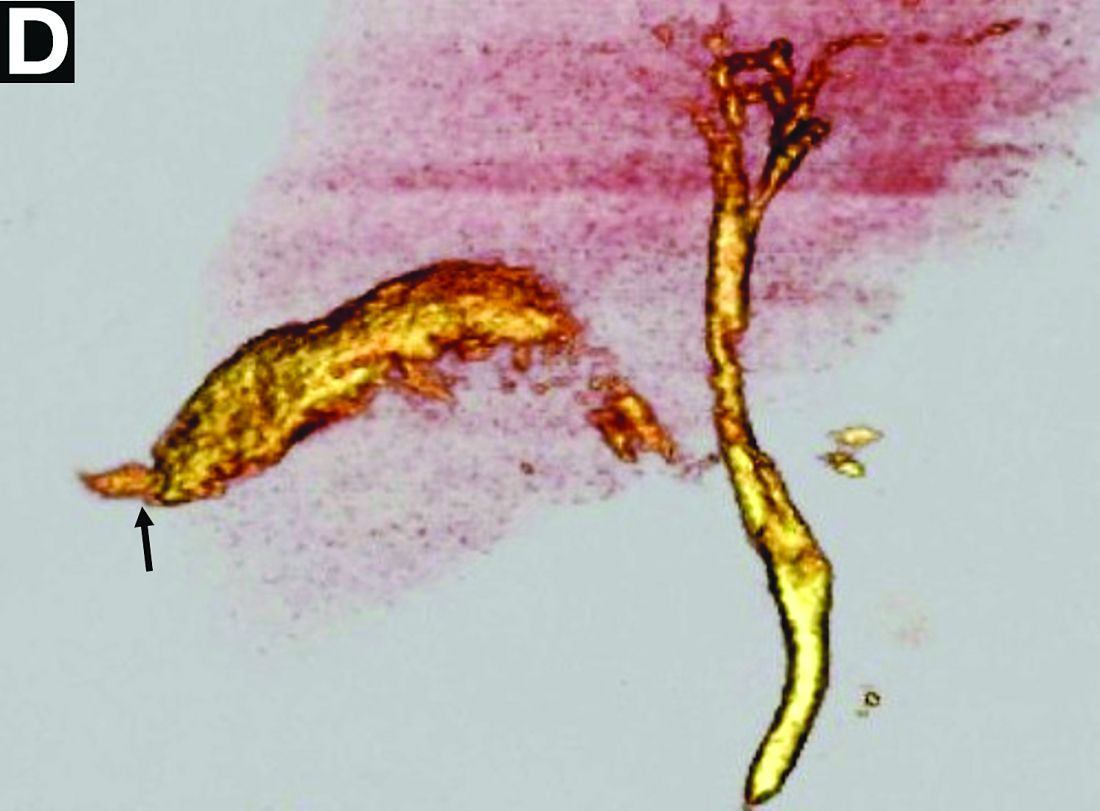
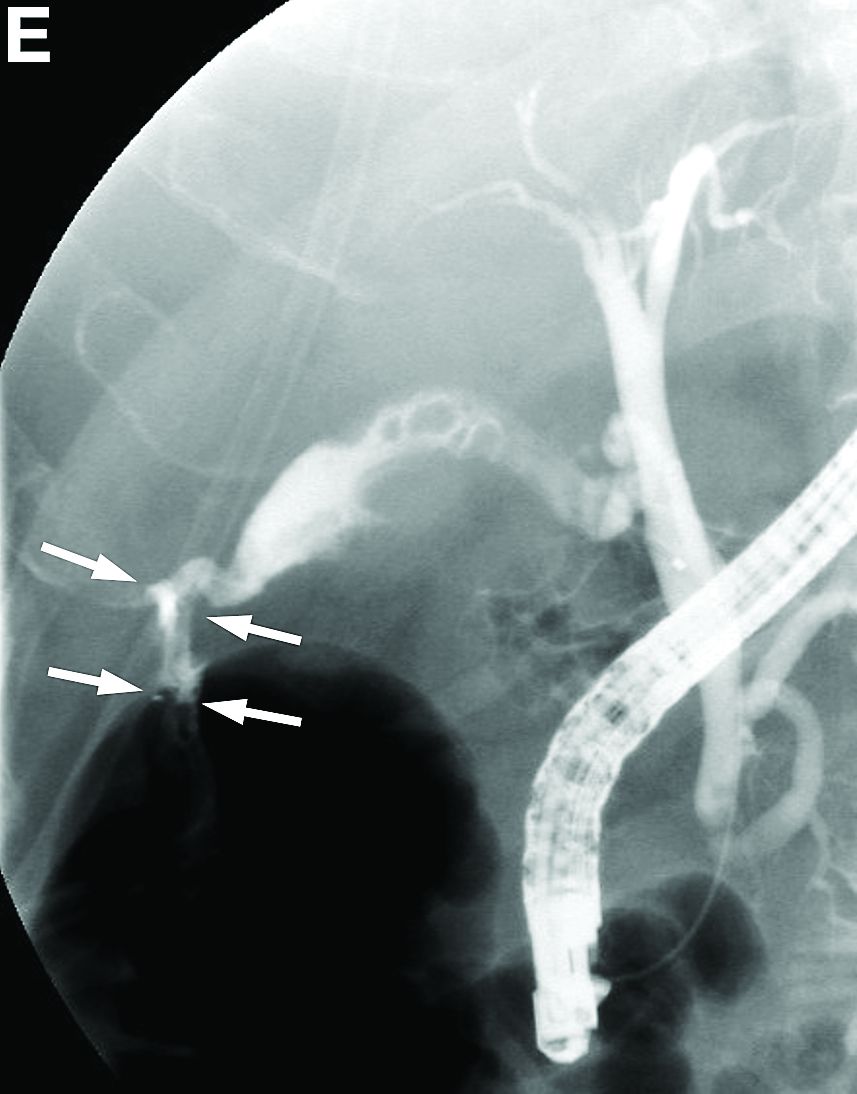
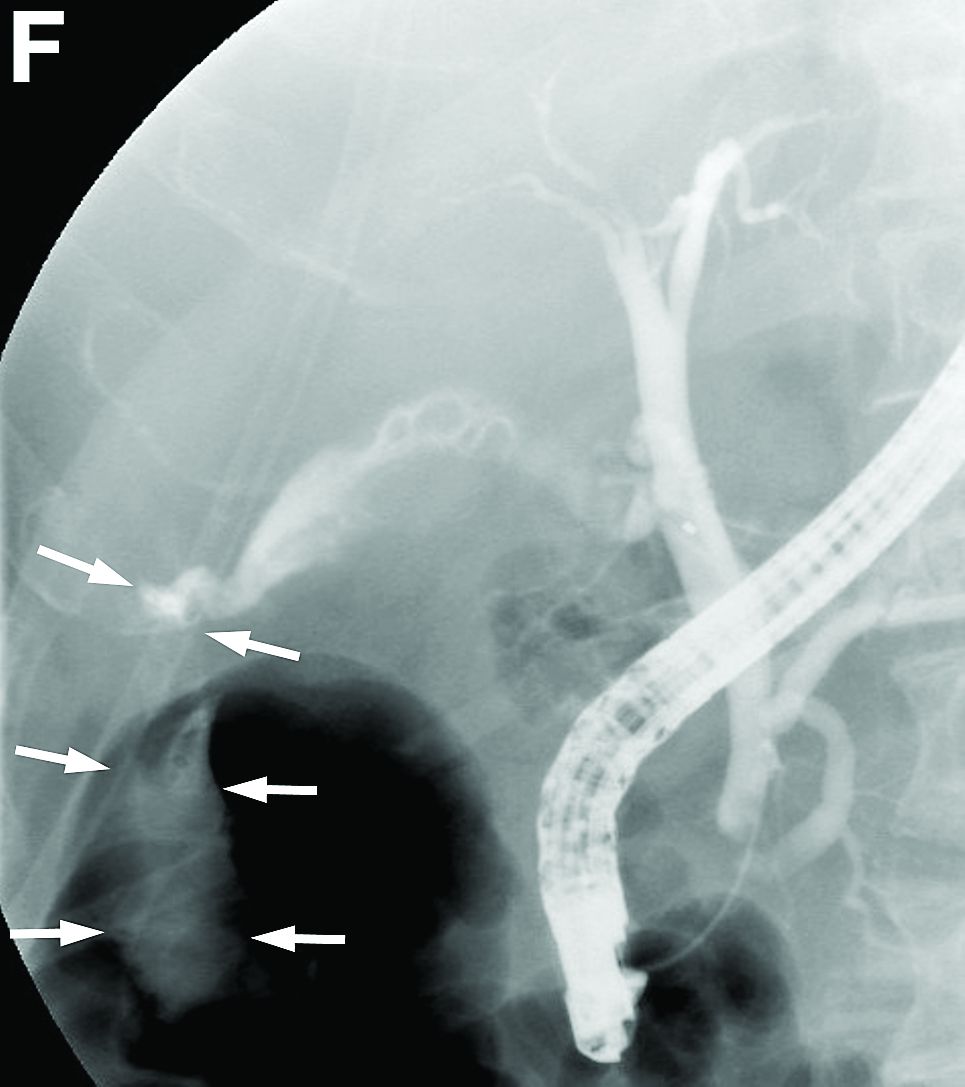
No definite site of perforation was observed in the biliary tract by CT. However, with a suspicion of biliary tract perforation, 3-dimensional drip-infusion CT cholangiography was performed, which revealed a leakage of contrast medium from the gallbladder fundus (Figure D, arrow) into the subhepatic space, leading to a diagnosis of spontaneous gallbladder perforation. Endoscopic retrograde cholangiography confirmed the perforation at the same site (Figure E, F, arrows). An endoscopic nasobiliary drainage tube was placed, and bile was aspirated continuously. Four weeks later, when the general condition of the patient stabilized, cholecystectomy was performed. Histologic examination showed a 3-mm perforation in the gallbladder fundus with marked necrosis of the gallbladder wall associated with chronic cholecystitis. No stones were found. He had an uneventful recovery and was discharged in an improved condition.
Gallbladder perforation is a rare but life-threatening complication of cholecystitis with or without stones, with a recently reported mortality rate of 9.5%.1 Niemeier2 classified the condition into three types: type I (acute), free perforation and generalized peritonitis; type II (subacute), localized peritonitis and pericholecystic abscess; and type III (chronic), cholecystoenteric fistula. These classifications are still in use. Our patient had a type I perforation. The most common site of perforation is the fundus because of its poor blood supply. Predisposing factors for spontaneous gallbladder perforation include cholelithiasis, infections, diabetes mellitus, atherosclerosis, and steroid therapy, which was observed in the present case.
The diagnosis is suggested by ultrasonography, CT, magnetic resonance imaging, endoscopic retrograde cholangiography, or cholescintigraphy. As observed in the present case, drip-infusion CT cholangiography provides high-quality images of the biliary system; however, the availability of intravenous cholangiographic contrast media is limited to a few countries.3 The difficulties in diagnosis cause a delay in treatment and lead to high morbidity and mortality. Gallbladder perforation should be considered as a differential diagnosis in patients presenting with peritonitis with an unknown etiology.
References
1. Ausania, F., Guzman Suarez, S., Alvarez Garcia, H. et al. Gallbladder perforation: morbidity, mortality and preoperative risk prediction. Surg Endosc. 2015;29:955-60.
2. Niemeier, O.W. Acute free perforation of the gall-bladder. Ann Surg. 1934;99:922-4.
3. Hyodo, T., Kumano, S., Kushihata, F. et al. CT and MR cholangiography: advantages and pitfalls in perioperative evaluation of biliary tree. Br J Radiol. 2012;85:887-96.