Obesity in the elderly: More complicated than you think





ABSTRACTThe number of obese older adults is on the rise, although we lack a proper definition of obesity in this age group. The ambiguity is primarily related to sarcopenia, the progressive loss of muscle and gain in fat that come with aging. Whether to treat and how to treat obesity in the elderly is controversial because of a paucity of established guidelines, but also because of the obesity paradox—ie, the apparently protective effect of obesity in this age group.
KEY POINTS
- In older patients, the waist circumference may be more appropriate than the body mass index as a measure of adiposity.
- Data suggest that being moderately overweight may offer a survival advantage in older people, but a body mass index of 30 kg/m2 or higher continues to be associated with many health risks in this age group.
- In obese patients, intensive lifestyle interventions with an emphasis on exercise and strength training can optimize their overall health and quality of life.
- Weight-loss recommendations in older obese patients should take into account the benefits and risks of lifestyle interventions, drug therapy, and bariatric surgery.
Possible explanations for the paradox
Several hypotheses have been proposed to explain the change in the relationship between BMI and the risk of death that occurs with aging.
The BMI is an imperfect measure of obesity. The obesity paradox may be an artifact of using the BMI to measure obesity in older adults.17 As described above, sarcopenic obesity must be considered in those over age 65 because the BMI does not differentiate between fat and muscle. Older adults tend to have a higher proportion of body and visceral fat that is distributed differently, making the waist circumference or waist-hip ratio a more appropriate measure of obesity in this group.38 Janssen et al39 found that in people age 65 and older, after controlling for waist circumference, higher BMI values were associated with lower death rates; after controlling for BMI, waist circumference was associated with a higher risk of death.
The survival effect suggests that people who are susceptible to the negative effects of obesity die sooner,40 and those who survive until old age may be resistant to the effects of obesity.41 If true, the survival effect would explain why the death rate seems to be unaffected by BMI in the older population.
Unhealthy weight loss. Smoking and diseases such as cancer that can cause early death may also induce weight loss, further complicating the relationship between BMI and death.19 After age 80, the association between BMI and the risk of death is weak because those with a low BMI include not only those who have always been lean and physically active, but also those who lost weight through chronic ill health or smoking.17
Further study needed. Thus, a number of confounding variables may muddy the association between obesity and death in older adults. Obesity should not be misinterpreted as being harmless or beneficial in older adults. Stevens et al36 found that a greater BMI was associated with a higher rate of death from all causes and from cardiovascular disease in men and women up to age 75, but that the relative risk of death associated with a greater BMI decreased with age.
Optimal BMI targets in older people have yet to be validated in a large prospective trial. However, multiple studies have examined the relationship between BMI and all-cause mortality in older adults and have identified a BMI of 24 to 35 as “ideal” and associated with the lowest risk of death, with a lower range for men and a higher range for women.42,43 The topic has been reviewed by Oreopoulos et al.26 More research is needed to evaluate this relationship.
THE BENEFIT OF WEIGHT LOSS IN OLDER ADULTS IS CONTROVERSIAL
In younger obese people, weight loss brings a multitude of benefits by reducing the risk of complications arising from obesity. However, in older adults, the effects of weight loss remain controversial, and evidence to guide treatment is limited.44,45 The few trials that have been published have typically focused on cardiovascular risk factors rather than physical function.45
In a 1-year trial, 107 people age 65 or older were randomized to a control group, to weight management, to exercise, or to weight management plus exercise. The combination of weight loss and exercise yielded the greatest improvement in physical function.46
Intentional vs unintentional weight loss
Intentional weight loss is altogether different from unintentional weight loss.
In most cases, weight loss in older adults is unintentional and may indicate underlying disease and impending death.17 For example, older men who lose weight unintentionally have significantly greater rates of smoking, disability, cancer, and respiratory disease and less obesity and physical activity than those who lose weight intentionally.47
Studies have shown an increase in life expectancy in older patients with type 2 diabetes mellitus who lost weight intentionally.48,49 In fact, moderate weight loss—just 5% to 10%—has been shown to improve cardiovascular risk factors,44 osteoarthritis, and type 2 diabetes.50
Bales and Buhr44 performed a systematic review of 16 studies that had lasted at least 6 months. Patients were age 60 or older with a minimum baseline BMI of 27 kg/m2 who intentionally lost at least 3% of body weight or 2 kg. Levels of the inflammatory markers C-reactive protein, tumor necrosis factor alpha, and interleukin 6 declined with weight, along with blood pressure, fasting glucose, waist circumference, and low-density lipoprotein cholesterol. On the downside, bone mineral density and lean body mass also declined slightly. The best way to avoid losing lean body mass and to preserve bone density during weight loss is to include a program of resistance-training exercises.
No clinical trial has evaluated the effects of intentional weight loss on death rates in older obese people.25 As a result, evidence-based recommendations cannot be made. Rather, advice on weight loss must be individualized, with special emphasis on the patient’s weight history and medical comorbidities.44
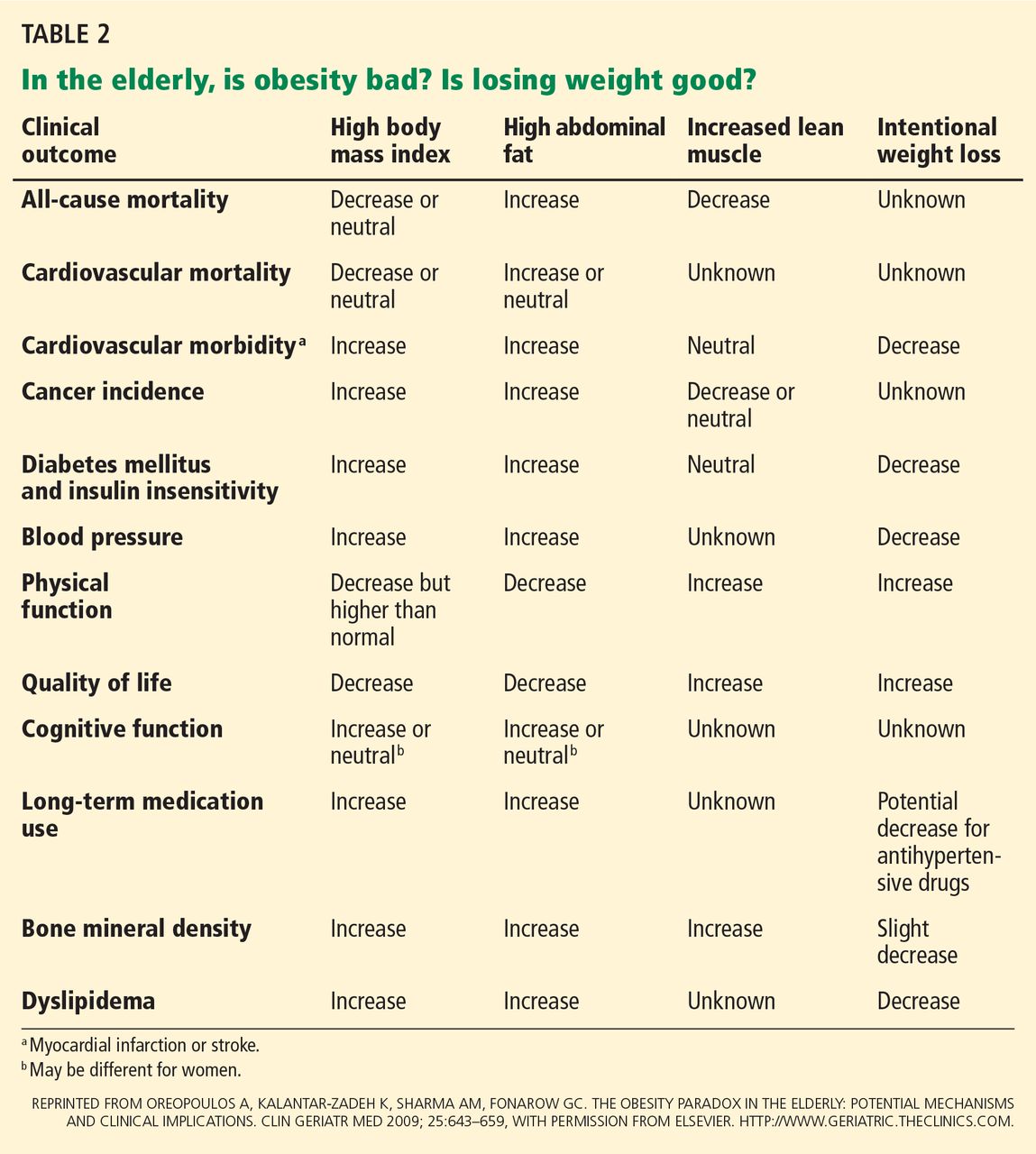
Oreopoulos et al26 summarized the possible effects of BMI, abdominal fat, lean body mass, and intentional weight loss on morbidity and mortality outcomes in older adults (Table 2).
TREATMENT GUIDELINES AND RECOMMENDATIONS
Many of the methods of weight management in older adults are the same as in young and middle-aged adults.51 Recommendations for all age groups include lifestyle changes, increased activity, dietary changes, drug therapy, and bariatric surgery.
Whether there should be separate guidelines for older adults is controversial. In view of the obesity paradox, physicians have been reluctant to recommend weight loss in elderly patients. Caution is advised in recommending weight loss solely on the basis of body weight, as studies have shown that the weight associated with maximal survival increases with age. Because of age-related changes in body composition and reduced energy requirements and expenditure, recommendations for the young and middle-aged should not be applied directly to older adults.
In this group, especially those who have survived into old age with good health and an intact functional status, one could argue that significant caloric restriction should not be recommended. In these people, the goal is often to maintain weight and incorporate a daily exercise program rather than to aggressively lose weight. Adding resistance training can improve physical function, which can improve quality of life. There is less emphasis on cardiovascular risk, but both outcomes apply for both age groups.52
Intentional weight loss should be recommended to high-risk older adults, including those with cardiovascular disease, type 2 diabetes mellitus, and metabolic syndrome, because the absolute risk of death and morbidity is higher in this group. Most health benefits can be achieved with modest weight loss.53 Potential benefits include prevention of cognitive impairment, protection from bone fractures, an increase in antioxidant defense, a reserve of fat and energy stores, and an increase in longevity.26
Treatment differs from that in the younger population primarily because of the importance of preventing loss of muscle with intentional weight loss. People of all ages who lose weight intentionally lose fat and, to a lesser extent, skeletal muscle. Older patients have already lost muscle mass, but further changes in body composition, especially a further reduction in muscle mass, can be limited by consuming about 1.0 g/kg of high-quality protein in the diet and by engaging in resistance training and weight training.52
Improving quality of life and physical function are important goals. Information is emerging about when obesity needs to be managed in older adults. There is also evidence to support dietary and exercise therapy.54 Weight-loss options include lifestyle interventions, pharmacotherapy, and bariatric surgery.