Innovative models of home-based palliative care





ABSTRACTThe focus of palliative care is to alleviate pain and suffering for patients, potentially while they concurrently pursue life-prolonging or curative therapy. The potential breadth of palliative care is recognized by the Medicare program, but the Medicare hospice benefit is narrowly defined and limited to care that is focused on comfort and not on cure. Any organization or setting that has been accredited or certified to provide health care may provide palliative care. Home health agencies are highly attuned to patients’ need for palliative care, and often provide palliative care for patients who are ineligible for hospice or have chosen not to enroll in it. Two home health–based programs have reported improved patient satisfaction, better utilization of services, and significant cost savings with palliative care. Moving the focus of care from the hospital to the home and community can be achieved with integrated care and can be facilitated by changes in government policy.
WHAT IS HOME HEALTH’S ROLE IN PROVIDING PALLIATIVE CARE?
Many Medicare-certified home health agencies also operate Medicare-approved hospice programs. Home health agencies have a heightened perspective on patients’ palliative care needs. Because of the limited nature of the Medicare hospice benefit, home health agencies have built palliative care programs to fill unmet patient needs. Home health agencies often provide palliative care to patients who may be ineligible for the hospice benefit or have chosen not to enroll in it. These programs are particularly attractive to patients who would like to pursue curative treatment for their serious illnesses or who are expected to live longer than 6 months.
Home health patients with advancing or serious illness or chronic illness are candidates for a palliative care service. For these patients, the burden of their illness continues to grow as distressing symptoms begin to more regularly impact their quality of life. As they continue curative treatment of their illness, they would benefit from palliative care services that provide greater relief of their symptoms and support advanced care planning. Palliative care interventions become an integrated part of the care plan for these patients. Home health agencies serving patients with chronic or advancing illnesses will see care benefits from incorporating palliative care into their team’s skill set.
Two innovative examples of home health–based programs that include a palliative care component have been reported in peer-reviewed literature to date: Kaiser Permanente’s In-Home Palliative Care program and Sutter Health’s Advanced Illness Management (AIM) program.7–10
Kaiser Permanente’s In-Home Palliative Care Program
Kaiser Permanente (KP) established the TriCentral Palliative Care Program in 1998 to achieve balance for seriously ill patients facing the end of life who were caught between “the extremes of too little care and too much.”11 KP began the program after discovering that patients were underusing their existing hospice program. The TriCentral Palliative Care program is an outpatient service, housed in the KP home health department and modeled after the KP hospice program with three key modifications designed to encourage timely referrals to the program:
- Physicians are asked to refer a patient if they “would not be surprised if this patient died in the next year.” Palliative care patients with a prognosis of 12 months or less to live are accepted into the program.
- Improved pain control and symptom management are emphasized, but patients do not need to forgo curative care as they do in hospice programs.
- Patients are assigned a palliative care physician who coordinates care from a variety of health care providers, preventing fragmentation.
The program has five core components that are geared toward enhanced quality of care and patient quality of life. These core components are:
- An interdisciplinary team approach, focused on patient and family, with care provided by a core team consisting of a physician, nurse, and social worker, all with expertise in pain control, other symptom management, and psychosocial intervention
- Home visits by all team members, including physicians, to provide medical care, support, and education as needed by patients and their caregivers
- Ongoing care management to fill gaps in care and ensure that the patient’s medical, social, and spiritual needs are being met
- Telephone support via a toll-free number and after-hours home visits available 24 hours a day, 7 days a week as needed by the patient
- Advanced-care planning that empowers patients and their families to make informed decisions and choices about end-of-life care11
Assessments of the program’s results in a randomized controlled trial8 and a comparative study9 showed that patient satisfaction increased; patients were more likely to die at home in accordance with their wishes; and emergency department (ED) visits, inpatient admissions, and costs were reduced (Table 1).
Sutter Health AIM Program
Sutter Health in northern California, in collaboration with its home care and hospice affiliate, Sutter Care at Home, initiated a home health–based program, Advanced Illness Management (AIM), in 2000 in response to the growing population of patients with advanced illness who needed enhanced care planning and symptom management. This program served patients who met the Medicare eligibility criteria for home health, had a prognosis of 1 year or less, and were continuing to seek treatment or cure for their illness. These patients frequently lacked awareness of their health status, particularly as it related to choices and decisions connected to the progression and management of their conditions. They also were frequently receiving uncoordinated care through various health channels, resulting in substandard symptom management. As a result, patients tended to experience more acute episodes that required frequent use of “unwanted and inappropriate care at the end of life, and they, their families, and their providers were dissatisfied.”12
As the AIM program matured, it incorporated a broader care management model, including principles of patient/caregiver engagement and goal setting, self-management techniques, ongoing advanced care planning, symptom management, and other evidence-based practices related to care transitions and care management. The program connects with the patient’s network of care providers and coordinates the exchange of realtime information about the current status of care plans and medication, as well as the patient’s defined goals. This more comprehensive model of care for persons with advanced illness has achieved improved adherence to patient wishes and goals, reductions in unnecessary hospital and ED utilization, and higher patient/caregiver and provider satisfaction than usual care.
Today, AIM is not primarily a palliative care program. Rather, it provides a comprehensive approach to care management that moves the focus of care for advanced illness out of the hospital and into the home/community setting. AIM achieves this through integrating the patient’s “health system.”
This integration occurs through formation of an interdisciplinary team comprised of the home care team, representative clinicians connected to the hospital, and providers of care for the patient. This expanded team, then, becomes the AIM care management team that is trained on the principles of AIM and its interventions. With this enhanced level of care coordination and unified focus on supporting the patient’s personal health goals, the AIM program serves as a “health system integrator” for the vulnerable and costly population of people with advanced chronic illness.
Inpatient palliative care is a separate and distinct systemwide priority at Sutter Health and, because of this, AIM collaborates closely with the inpatient palliative care teams to ensure that patients experience a seamless transition from hospital to home. There, AIM staff work with patients and families over time to clarify and document their personal values and goals, then use these to develop and drive the care plan. Armed with clearer appreciation of the natural progression of illness, both clinically and practically, coupled with improved understanding of available options for care, most choose to stay in the safety and comfort of their homes and out of the hospital. These avoided hospitalizations are the primary source of AIM’s considerable cost savings.
Patients eligible for AIM are those with clinical, functional, or nutritional decline; with multiple hospitalizations, ED visits, or both within the past 12 months; and who are clinically eligible for hospice but have chosen to continue treatment or have not otherwise made the decision to use a hospice model of care. Once the patient is enrolled, the AIM team works with the patient, the family, and the physician on a preference-driven plan of care. That plan is shared with all providers supporting the patient and is regularly updated to reflect changes in the patient’s evolving choices as illness advances. This tracking of goals and preferences over time as illness progresses has been a critical factor in improving outcomes, especially those related to adherence or honoring a patient’s personal goals.
The AIM program started as a symptom management and care planning intervention for Medicare-eligible home health patients. The program has evolved over time into a pivotal fulcrum by which to engage or create an interdisciplinary focus and skill set across sites and providers of care in an effort to improve the overall outcomes for patients with advancing illness. In 2009, the AIM program began geographically expanding its home health–based AIM teams across 12 counties surrounding the San Francisco Bay area and the greater Sacramento region in northern California. The program now coordinates care with more than 17 hospitals and all of the large Sutter-affiliated medical groups, and it serves approximately 800 patients per day.
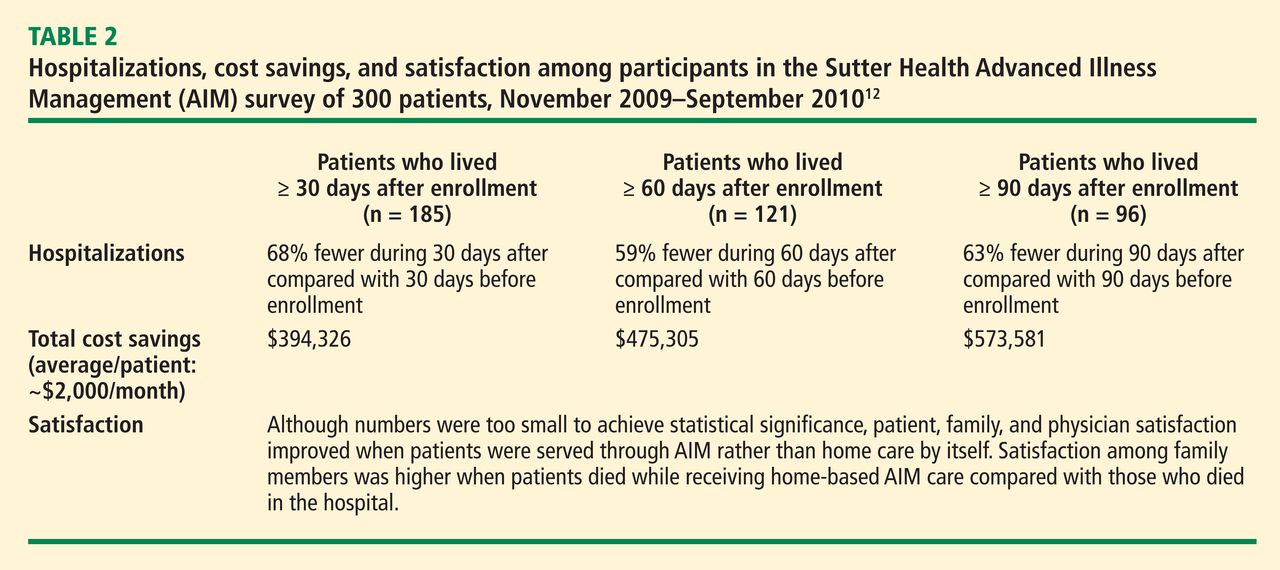
The AIM program has yielded significant results in terms of both quality of care and cost savings. Preliminary data on more than 300 AIM patients surveyed from November 2009 through September 2010 showed significant reductions in unnecessary hospitalizations and inpatient direct care costs (Table 2).12 Survey data also showed significant improvements in patient, family, and physician satisfaction when late-stage patients were served through AIM rather than through home care by itself.12
The Sutter Health AIM program recently received a Health Care Innovation Award from the Center for Medicare & Medicaid Innovation (CMMI) because of the program’s ability to “improve care and patient quality of life, increase physician, caregiver, and patient satisfaction, and reduce Medicare costs associated with avoidable hospital stays, ED visits, and days spent in intensive care units and skilled nursing facilities.”13 The $13 million CMMI grant will help expand AIM to the entire Sutter Health system. It is estimated that the program will save $29,388,894 over 3 years.13