Preserving fertility in female cancer patients: A snapshot of the options





ABSTRACTWith the odds of surviving cancer improving, many young women facing chemotherapy or radiotherapy may first wish to take steps to ensure that they will still be able to bear children afterward. The options depend on the type of disease, the treatment required, the age of the patient, whether she has a long-term partner, and whether cancer treatment can be delayed. This paper is an overview of current and experimental strategies for preserving fertility in female cancer patients.
KEY POINTS
- Chemotherapy and radiotherapy are toxic to the ovaries, although the damage can be attenuated in some cases.
- The standard option for preserving fertility has been oocyte retrieval after controlled ovarian stimulation, followed by in vitro fertilization and subsequent cryopreservation of the resulting embryos.
- Unfortunately, controlled ovarian stimulation takes time, may delay needed cancer therapy, and may worsen estrogen-dependent cancers. Alternatives are being explored.
- Cryopreservation of unfertilized oocytes is an option for women who do not have a partner, although oocytes are more susceptible to damage during freezing than embryos are.
HOW CANCER TREATMENT DAMAGES THE OVARIES
Advances in surgery, radiotherapy, and chemotherapy have significantly improved the prognosis for young cancer patients. However, cancer treatments often result in ovarian dysfunction, and premature menopause and irreversible sterility are the most dramatic outcomes. The resulting low estrogen levels, in addition to their physiologic consequences, also worsen quality of life through psychological effects, which can as well influence the patient’s compliance with treatment.
Chemotherapy: Alkylating agents are the most gonadotoxic
The mechanism by which chemotherapy affects ovarian function is poorly understood. Histologically, chemotherapeutic drugs could lead to ovarian atrophy and stromal fibrosis, to depletion of the primordial follicle stockpile, and to reduced ovarian weight, resulting in ovarian dysfunction.5
The patient's age correlates with the probability of ovarian damage or, inversely, ovarian resistance to chemotherapy. Young women have more primordial oocytes, and after chemotherapy they face a sharp reduction of their ovarian reserve. Still, younger patients show a lower rate of ovarian toxicity than older women.6
The type and the cumulative dose of cytotoxic agents used are other important variables.7 There are six main classes of chemotherapeutic drugs: alkylating agents, platinum derivatives, antibiotics, antimetabolites, plant alkaloids, and taxanes. They all affect ovarian function, but alkylating agents are the most gonadotoxic.
Alkylating agents covalently bind an alkyl group to the DNA molecule and inhibit it from replicating. In the ovaries they directly injure primordial oocytes and deplete follicles. 8 They also seriously damage the ovarian vasculature so that the follicles cannot grow.9 Their destructive effect on the primordial follicles is dose-dependent and varies with the age and developmental maturity of the patient at the time of the therapy, with older women more likely to be left infertile afterward.10
Cyclophosphamide is an alkylating agent often used to treat severe manifestations of autoimmune diseases such as systemic lupus erythematosus, BehÇet disease, steroid-resistant glomerulonephritis, inflammatory bowel disease, pemphigus vulgaris, and others. Because it can lead to premature ovarian failure and infertility, women receiving cyclophosphamide for autoimmune conditions may also need treatment to preserve fertility.11
Radiotherapy
Ovarian follicles are remarkably vulnerable to damage from ionizing radiation, which results in ovarian atrophy and reduced follicle stores.1
The risk of radiotherapy-induced infertility is closely related to the patient’s age and developmental maturity at the time of therapy and to dose fractionation and the extent of the irradiation field. Every patient has a different sensitivity to radiation damage that is probably genetically predetermined, but age seems to be the most important variable. Wo and Viswanathan12 used a mathematical model devised by Wallace et al13 to show that the older the patient, the lower the radiation dose necessary to impair ovarian function.
The irradiation field is another aspect to consider. Pelvic radiation can be necessary in rectal cancer, cervical cancer, and lymphoma. In these cases, surgically moving the ovaries to a region outside the radiation field could be an option to minimize radiotherapy-induced ovarian damage.14
Radiotherapy can also damage the uterus. Pelvic irradiation can reduce uterine volume, alter uterine elasticity through myometrial fibrosis, and modify vascularization and endometrial thickness.15,16 These alterations are closely correlated with the total radiation dose, the site of irradiation, and the patient’s age at the time of the treatment, the prepubertal uterus being more susceptible to damage. 15,17 Larsen et al15 found that girls who received uterine irradiation before puberty had lower uterine volumes in adulthood than girls who received chemotherapy alone or radiation to other parts of the body, and that the younger the patient at the time of radiotherapy, the smaller the uterus later. These effects could result in adverse pregnancy outcomes.
Furthermore, radiation could also damage the uterine vasculature. Holm et al16 used ultrasonography to evaluate the effect of total-body irradiation and found that uterine volume and uterine blood flow were both impaired.15
All these possible alterations could lead to a reduced uterine response to cytotrophoblast invasion and to decreased fetoplacental blood flow, which could impair embryonic and fetal growth. In that case, a surrogate pregnancy would be the only method to achieve parenthood using the couple’s gametes.
OPTIONS FOR FERTILITY PRESERVATION
Assisted reproductive technology
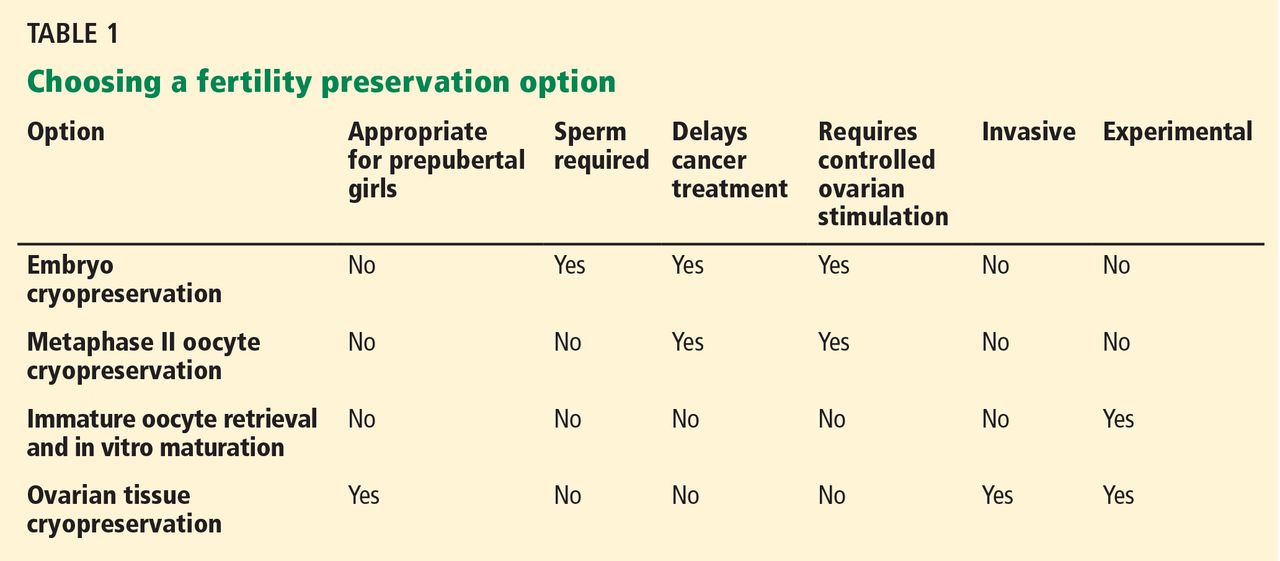
Young women diagnosed with an oncologic disease may wish to use assisted reproductive technology (Table 1) to keep open the possibility of having children at a later date. One approach is to harvest oocytes, fertilize them in vitro, and deep-freeze (cryopreserve) the resulting embryos to be thawed and implanted later. Alternatively, oocytes can be frozen directly, although success rates are lower with this method. And another approach is to obtain and cryopreserve ovarian tissue. If none of these is possible, oocytes may be obtained from a donor.
Controlled ovarian stimulation
If oocytes are to be harvested, a number of them should be harvested at one time.
There is not an optimal number of oocytes that should be retrieved, but cryopreservation of a large number of oocytes allows us to perform multiple attempts at in vitro fertilization, improving the chances of pregnancy. The fertilization rate (defined as the total number of zygotes at the 2-pronucleus stage divided by the number of fertilized oocytes) with intracytoplasmic sperm injection is 70% to 80%. On average, for every 10 eggs, 7 to 8 eggs will normally be fertilized. The implantation rate (defined as the total number of pregnancies divided by the total number of embryo transferred) with intracytoplasmic sperm injection is 40% to 50%—ie, only half of the transferred embryos will successfully implant and result in a pregnancy.
So that more than one ripe egg can be obtained at a time, the patient must undergo a regimen of controlled ovarian stimulation to achieve multifollicular growth. Stimulation protocols are based on giving pituitary hormones, ie, analogues of gonadotropin-releasing hormone (GnRH) (both agonists and antagonists), followed by recombinant FSH or human menopausal gonadotropin to promote follicular development. A single dose of human chorionic gonadotropin (hCG) is given to induce ovulation when the lead follicles have reached 18 to 20 mm in size.18
Many oncologists consider controlled ovarian stimulation dangerous for cancer patients because it takes time and thus delays cancer treatment. Furthermore, the regimen boosts the levels of circulating estrogens, which could be harmful in patients with hormone-dependent tumors.19
Oocytes can also be retrieved during unstimulated cycles. This avoids increasing estrogen concentrations above the physiologic level, but no more than a single oocyte is collected per cycle. The patient could undergo multiple oocyte harvestings, one per cycle, but this would delay her cancer treatment even more—by months—which is not recommended.
Serious efforts to minimize estrogen production during controlled ovarian stimulation have been made, although further studies are needed. Research is under way to develop appropriate ovarian stimulation protocols based on drugs with antiestrogenic effects.
Tamoxifen, an antagonist of the estrogen receptor, is widely used in breast cancer treatment. 20 It can also be given during controlled ovarian stimulation because it promotes follicular growth and induces ovulation.21 Oktay et al22 found that the embryo yield was 2.5 times higher in women with breast cancer treated with tamoxifen than in a retrospective control group consisting of breast cancer patients attempting natural-cycle oocyte retrieval.
Letrozole, an aromatase inhibitor, is also commonly used in treating breast and ovarian cancer. Aromatase is an enzyme that catalyzes the conversion of androgenic precursors to estrogens, and it is found in many tissues, including granulosa cells. Several studies report the use of letrozole, alone or in combination with low doses of recombinant FSH, in ovarian stimulation protocols in cancer patients, with positive clinical outcomes.23
Tamoxifen or letrozole, combined with recombinant FSH, is an attractive option in a controlled ovarian stimulation protocol for cancer patients,24 although further investigation is needed.