A practical guide to prostate cancer diagnosis and management





ABSTRACTScreening, diagnosis, and management of prostate cancer can be complicated, with no clear consensus about key issues. We present our approach, which reflects the guidelines of the American Urological Association (AUA).
KEY POINTS
- The AUA recommends annual screening with both digital rectal examination (DRE) and prostate-specific antigen (PSA) testing starting at age 40 for all men whose life expectancy is more than 10 years. Guidelines from other organizations differ somewhat.
- If the DRE is abnormal or if the PSA level is persistently higher than 2.5 μg/L, then biopsy should be considered.
- In low-risk cases, active surveillance may be acceptable in lieu of immediate treatment. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.
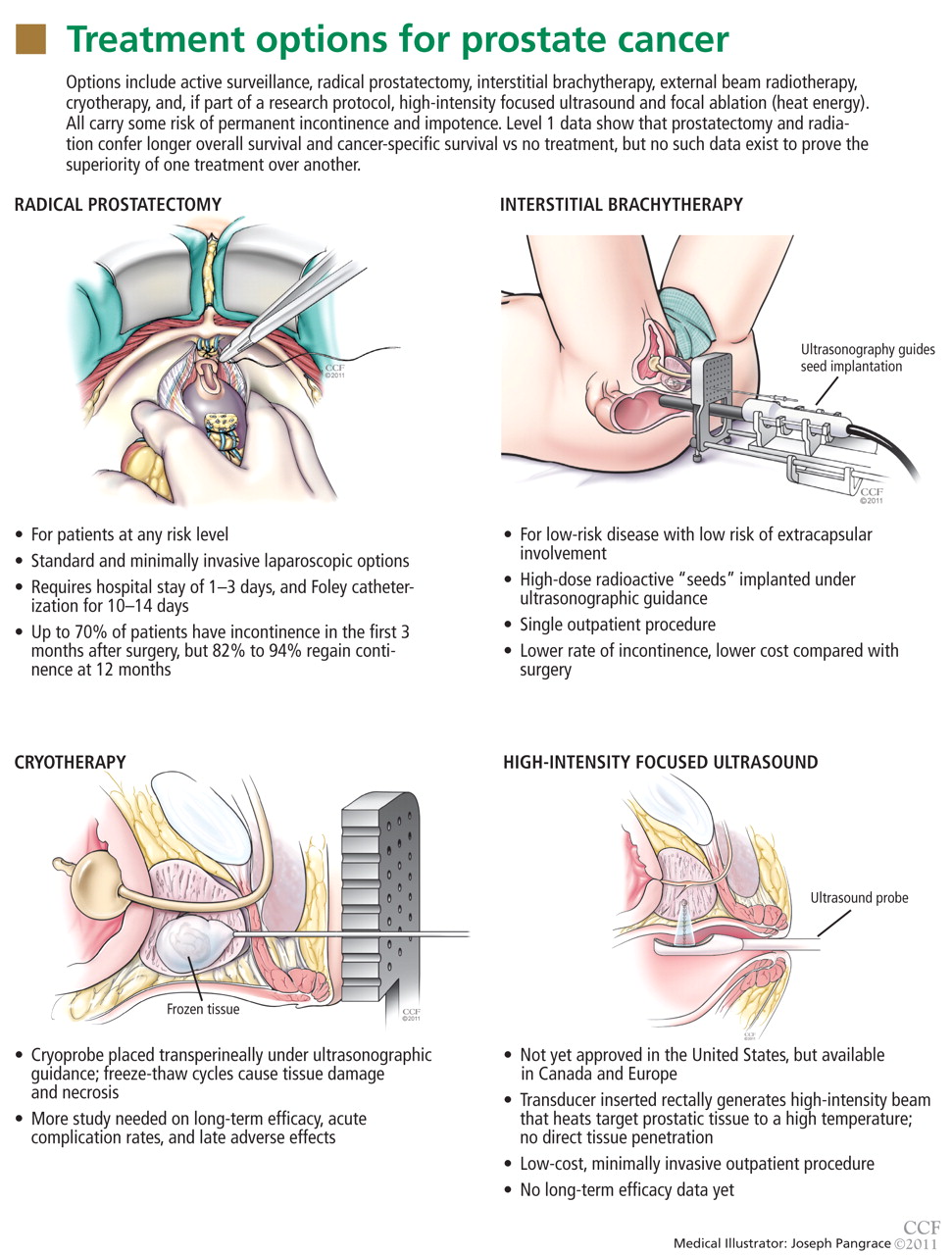
- The most common primary treatments are active surveillance, prostatectomy, interstitial brachytherapy, external beam radiotherapy, and cryotherapy. Newer ablative and focal therapies may offer an advantage in select patients. Which treatment to use is highly patient-dependent.
- Single-institution, single-surgeon reports and advertisements tend to underestimate rates of impotence after prostatectomy, and as a result patients may have false expectations.
BIOPSY IS INDICATED IF EITHER TEST IS ABNORMAL
In the past, imaging of the prostate with transrectal ultrasonography was used as a screening tool to detect prostate cancer. Further research showed that only 15% to 20% of hypoechoic lesions detected on ultrasonography contained cancer.8 Because of its low sensitivity and specificity, primary ultrasonographic screening (ie, transrectal ultrasonography alone) is not acceptable for screening or for diagnosis. Its main role is in guiding prostate biopsy.
Biopsy of the prostate with transrectal ultrasonographic guidance is indicated if either the DRE or the PSA level is abnormal. The standard of care is to use an 18-gauge biopsy needle-gun to obtain two to three tissue samples from each of six regions of the prostate, focusing on the outer peripheral zone, specifically the right and left bases, the mid-gland, and the apex.
Pathologic analysis of each tissue core takes into consideration the presence or absence of cancer, the Gleason score, and the percentage of the tissue sample volume that is occupied by cancer.
The Gleason grading system is based on the histologic appearance and reflects the degree of differentiation and aggressiveness of the cancer. The two most prominent tumor grades present are added to give a final Gleason score. For instance, a Gleason grade of 4+3=7 indicates a tumor with predominant Gleason grade 4 disease with a lesser amount of grade 3 disease. The number of positive core samples and the volume of cancer provide information on the severity of the cancer.
If the PSA is high but biopsy is negative
Prostate biopsy misses up to 30% of small cancers. Many of these are clinically insignificant, but about 20% of those missed cancers can be high-risk and thus merit identification. There should be a low threshold for repeating biopsy 1 year later in men who have a persistently high PSA or a rising PSA.
High-grade prostatic intraepithelial neoplasia is a common finding on biopsy. The incidence of de novo prostate cancer at 5 years in men with this finding is 22% to 26%.9 Patients with multifocal high-grade prostatic intraepithelial neoplasia should be monitored with PSA testing and DRE every 6 to 12 months and should be considered for repeat “saturation” biopsy (ie, obtaining as many as 36 core samples).
IF CANCER IS FOUND, HOW RISKY IS IT?
Patients with a new diagnosis of prostate cancer must decide on a treatment plan. This decision is highly individualized, based on the patient’s personal preferences, lifestyle, performance status (ie, his general well-being), disease severity, continence status, and sexual function.
When counseling patients about their disease and the treatment options, we consider three main factors:
- The severity of disease on biopsy
- The patient’s current state of health and performance status
- The patient’s understanding of and willingness to accept the adverse effects of the various treatments.
Pathologic features, the PSA level, and clinical stage determined by DRE are used to predict the severity of disease. Most data on the efficacy of treatments for prostate cancer are based on the incidence of biochemical recurrence, ie, a rise in PSA level after primary therapy. The AUA and the D’Amico risk criteria use biopsy pathology, clinical stage, and the pretreatment PSA level to predict the likelihood of biochemical recurrence (Table 1).10,11
DISCUSSING TREATMENT OPTIONS WITH THE PATIENT
In our practice, we usually do not recommend treatment in men with low-risk or intermediate-risk prostate cancer who have a life expectancy of less than 10 years, as most of them will likely die of a cause other than prostate cancer. For patients with poor baseline performance status, surveillance or radiation therapy may be preferable to surgery. In younger patients, surgery may confer a more durable benefit.
- No prospective, randomized clinical trials have directly compared these treatments
- Prostate cancer progresses slowly
- Definitions of treatment failure used in various studies have been inconsistent
- Clinical studies have been subject to selection bias.
ACTIVE SURVEILLANCE IS ACCEPTABLE FOR LOW-RISK PROSTATE CANCER
Active surveillance is an acceptable option for patients with low-risk prostate cancer (ie, if the Gleason score is ≤ 6, the tumor stage is T1c or T2a, and the PSA level is ≤ 10 μg/L). To rule out high-risk disease before starting a program of surveillance, repeat biopsy is advisable, although optional.
Active surveillance consists of PSA testing and DRE every 6 to 12 months, followed by repeat biopsy if significant changes are noted in either test. Some centers advocate biopsy with transrectal ultrasonographic guidance every year regardless of the PSA or DRE findings.
Whether a change in the PSA level is significant is subjective, but a recent phase 2 study in 453 patients23 on a program of active surveillance used a PSA doubling time of less than 3 years as a criterion for repeat biopsy. Thirty-eight percent of the men had to undergo radiation therapy or surgery within 10 years, and 5 patients (1%) died of prostate cancer. The authors concluded that active surveillance did not put these patients at undue risk, and that this approach prevented overtreatment of clinically insignificant prostate cancer.23
The risks of surveillance include the chance that cancer could progress to an incurable state during the surveillance period, greater anxiety for the patient, and, if prostatectomy becomes necessary, greater technical difficulty due to scarring from repeat biopsies. The benefit is postponement or complete avoidance of the adverse effects of treatment.
Debate continues over the potential dangers of deferred treatment of prostate cancer, but in certain patients it is an acceptable option. Patient education, accurate disease assessment, and compliance with monitoring are critical considerations.