Advance care planning: Beyond the living will





ABSTRACTFor a variety of reasons, the most commonly used advance directive documents (eg, the living will) may not be very useful in many situations that older adults encounter. The durable power of attorney for health care is a more versatile document. We advocate focusing less on “signing away” certain interventions and more on clarifying the goals of care in the ambulatory setting.
KEY POINTS
- In the ambulatory setting, start by assessing the patient’s prognosis and his or her receptiveness to advance care planning.
- For a patient in declining health who is willing to participate in the care planning process, it may be useful to take a full values history and to review the goals of care.
- For a patient with advanced disease who is unable or unwilling to participate in advance care planning, a limited approach may be appropriate, ie, identifying a surrogate decision-maker and ascertaining how much flexibility the surrogate should have with health care decisions.
- Whatever the patient’s life expectancy and level of receptivity, brief, episodic discussions are more useful than a one-time description of available written advance directives.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
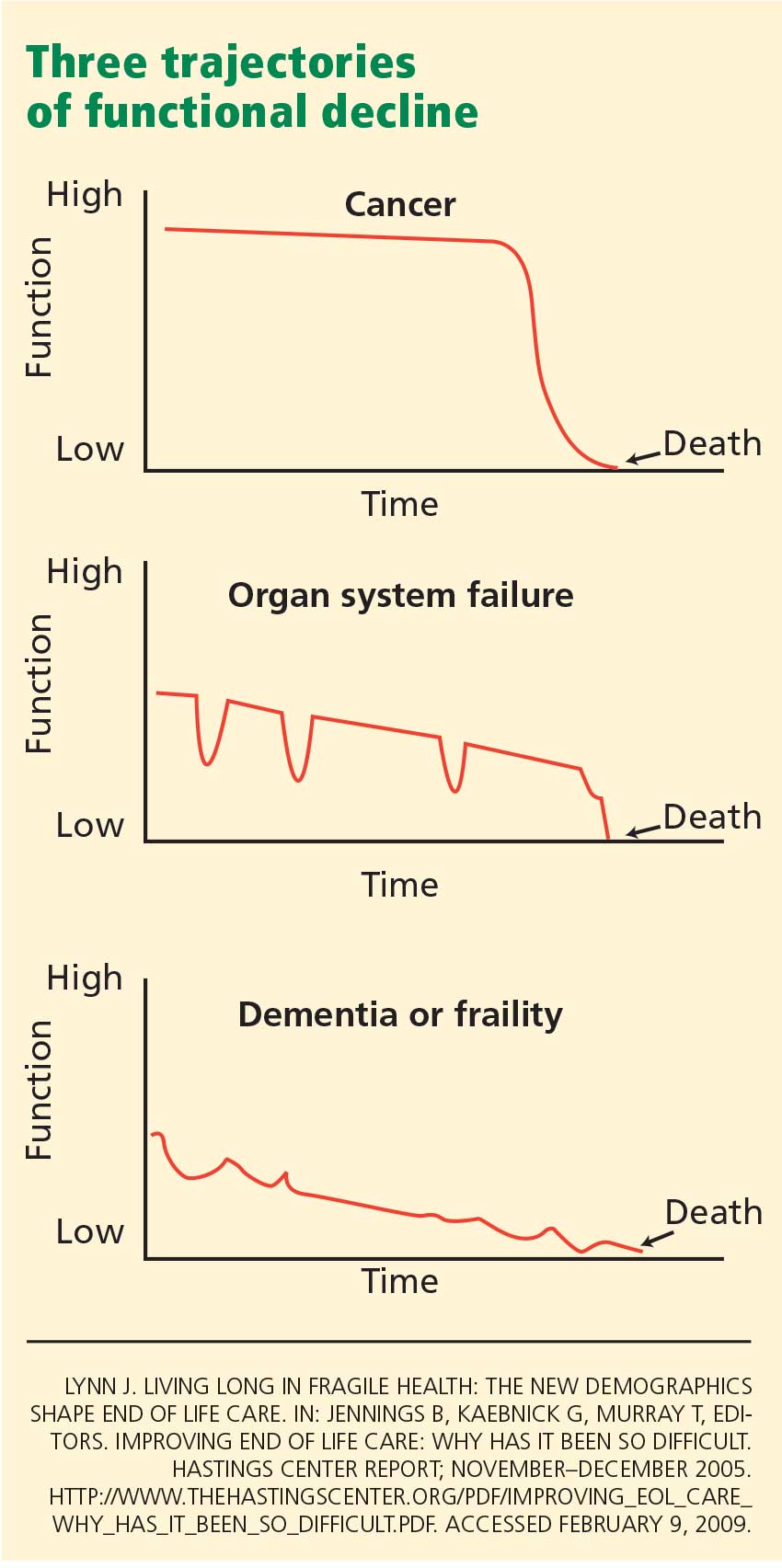
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.