The gout diagnosis





ABSTRACT
Synovial fluid aspiration and analysis is the gold standard for making the diagnosis of gout but is not always performed when indicated in clinical practice. In clinical situations when joint aspiration simply cannot be performed, a presumptive (or clinical) diagnosis of gout may be made in consultation with published recommendations and criteria from expert societies. A thorough patient history and physical examination are critical to a presumptive diagnosis of gout, as is serum urate measurement at the time of an acute attack and at follow-up 2 weeks later.
KEY POINTS
- If the serum urate level was not elevated when measured during an acute attack of arthritis, it will likely be elevated at 2-week follow-up if the patient does indeed have gout.
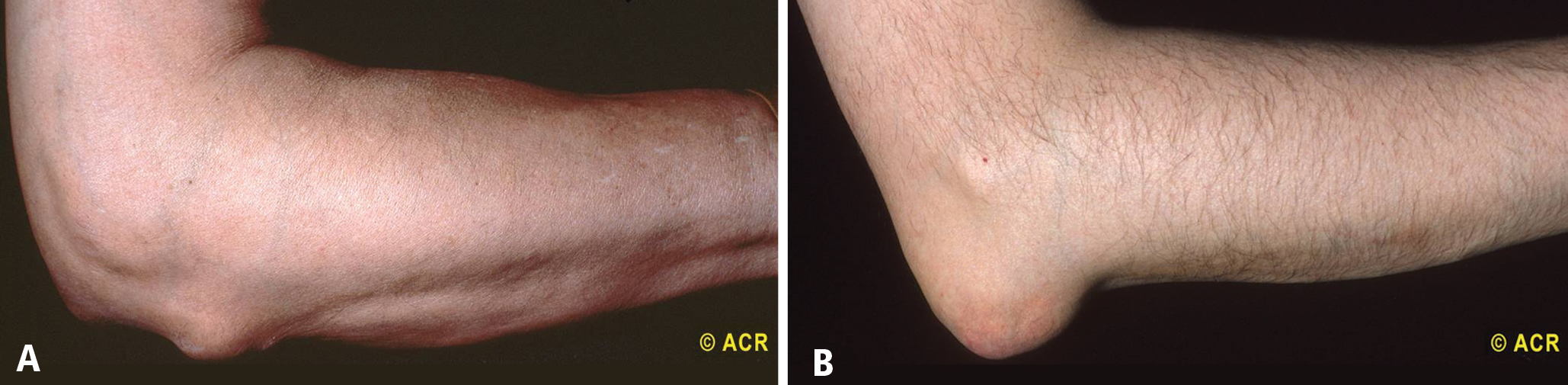
- Gouty tophi are typically found in the olecranon bursa, whereas rheumatoid nodules are usually located on the extensor surface of the forearm.
- Urate crystals of gout are negatively bifringent and fine and needlelike in shape, whereas the crystals of pseudogout are weakly positively birefringent and rhomboid.
- Gout and septic arthritis can coexist; when the differential diagnosis includes septic arthritis, joint aspiration is required.
- Until criteria for the presumptive diagnosis of gout are validated, clinicians should become familiar with the technique of joint aspiration.
SPECIAL CONSIDERATIONS FOR THE PRESUMPTIVE DIAGNOSIS OF GOUT
How long have acute attacks been occurring?
In a clinical scenario in which synovial fluid aspiration cannot be performed, the appropriateness of a presumptive diagnosis can be assessed by a discussion with the patient about how long he or she has been experiencing acute attacks of joint pain. If the attacks have occurred for more than 10 years, tophi will likely be present.3 After even longer periods, gout may become polyarticular.7 In postmenopausal women, the distal interphalangeal joints may be involved,3 which may lead to a misdiagnosis of osteoarthritis, as these joints are typically affected by osteoarthritis.
Is the patient taking a urate-raising medication?
Certain medications have been associated with hyper-uricemia, including cyclosporine and thiazide diuretics.9 If a patient has been taking one of these medications, gout should be considered in the differential diagnosis if the patient presents with acute joint pain.
It has been argued that a reduction in joint pain and swelling after the use of colchicine confirms a diagnosis of gout. However, other conditions—such as tendonitis, calcium pyrophosphate dihydrate (CPPD) crystal deposition disease (pseudogout),3 and rheumatoid arthritis (RA)—can also improve after treatment with colchicine.1
Be vigilant for fever
Another consideration in making a clinical diagnosis of gout is the association with a low-grade fever; these patients may feel as if they have the flu.8 Acute gout may also cause a high fever and an elevated white blood cell (WBC) count;3 in this situation, synovial fluid aspiration must be performed to exclude septic arthritis, either alone or in the presence of gouty arthritis. In situations where septic arthritis is suspected, an emergency visit to a rheumatologist is indicated for synovial fluid aspiration to be performed, as gout and sepsis can coexist.5 In such instances, Gram staining and culture of the synovial fluid should still be performed even if monosodium urate crystals are identified.5
MEASUREMENT OF SERUM URATE LEVELS
Measuring serum urate levels during an acute attack, treating the acute attack with anti-inflammatory medications, and reevaluating the patient in the office 2 weeks after the acute attack are all recommended in the management of a patient with gout. If the serum urate level was not elevated during the acute attack, it is likely to be elevated 2 weeks later if the patient has gout.10 Elevated levels of serum urate during the intercritical periods are predictive of future gout attacks.11 Measuring serum urate during the initial attack and then 2 weeks later yields two serum urate levels that can be compared to assist in considering a presumed diagnosis of gout. A study by Rigby and Wood concluded that in patients with low serum urate levels (< 4 mg/dL) 2 weeks following an inflammatory arthritis attack, a diagnosis of gout is unlikely.12
DIFFERENTIAL DIAGNOSIS OF GOUT
Rheumatoid arthritis
CPPD crystal deposition disease (pseudogout)
CPPD crystal deposition disease, or pseudogout, must also be included in the differential diagnosis of gout. This disease usually occurs in joints previously affected by osteoarthritis or joints that have been injured in the past.15 Attacks of CPPD crystal deposition disease commonly occur in the knee, in the wrist at the base of the thumb, or in the shoulder.15 Radiographic examination may reveal a line of calcification along the cartilage outlining the joint.15 Like gout, pseudogout attacks can occur spontaneously or after trauma, surgery, or a severe illness such as myocardial infarction or stroke.16
The presentation of pseudogout can be very similar to an acute attack of gout. The difference is seen when evaluating the crystals through a polarizing microscope. CPPD crystals are weakly positively birefringent (Figure 1B), in contrast to the negatively birefringent crystals seen with gout (Figure 1A).7 If a polarizing microscope is not available, the crystals usually can be distinguished by their differing shapes: urate crystals are fine and needlelike, whereas CPPD crystals are rhomboid (Figure 1).
Septic arthritis
When the differential diagnosis includes septic arthritis, the joint must be aspirated; a presumed diagnosis cannot be made. Among patients with an acute gouty attack, low-grade fever is reported during the attack in 29% of gout patients and 38% of patients with CPPD crystal deposition disease.14 Temperatures of 101°F or higher are not usually seen in patients with gout or CPPD crystal deposition disease and suggest an infection, although patients with septic arthritis may be afebrile, especially if they are taking immunosuppressive therapy or glucocorticoids, which can inhibit a febrile response. Synovial fluid analysis in patients with gout and septic arthritis can reveal WBC counts above 100,000 per mm3, whereas synovial fluid WBC counts above 50,000 per mm3 are more common in infection.
As noted earlier, gout and septic arthritis can coexist. In a patient presenting with a fever and a warm erythematous swollen joint, synovial fluid aspiration must be performed and evaluated for the presence of crystals and bacteria. The patient may require treatment for both causes of acute monoarticular arthritis.
In a patient undergoing renal dialysis, where gout or pseudogout can occur and where there is frequent intravascular manipulation, a septic joint can occur simultaneously.3,14 In this situation, not only must joint aspiration be performed, but the synovial fluid also needs to be evaluated for both crystals and bacteria. Again, the patient may require treatment for both causes of acute monoarticular arthritis.
CONCLUSIONS
The gold standard for diagnosing gout remains synovial fluid aspiration and analysis. In clinical situations when joint aspiration cannot be performed, the EULAR recommendations5 and the ACR criteria6 provide guidance for making a clinical or presumptive diagnosis of gout. A thorough patient history—both personal and family—and physical examination are critical in making a presumed diagnosis of gout. If the patient presents during an acute attack, serum urate measurement may be useful in making a clinical diagnosis if it reveals an elevated level. When the patient returns for follow-up 2 weeks later, a second serum urate measurement should be taken to allow comparison of the two levels. If the serum urate level is elevated at the follow-up visit, the EULAR recommendations state that a clinical diagnosis of gout can be made if the patient had an acute attack of arthritis in the great toe.
As noted in the EULAR recommendations, the future research agenda should include validating the clinical manifestations of gout against a diagnosis established by identification of urate crystals on synovial fluid analysis.5 Until this task can be completed, clinicians should become familiarized with the technique of joint aspiration so that in situations where a clinical or presumptive diagnosis of gout cannot be made—including cases where the differential diagnosis includes a septic joint—clinicians will be able to perform aspiration with confidence.