Cardiovascular autonomic dysfunction in patients with movement disorders





ABSTRACT
Autonomic dysfunction is common in parkinsonian syndromes, particularly those involving dysregulation of alpha-synuclein, and may result from neurodegeneration in autonomic regulatory regions of the brain or peripherial autonomic ganglia. The most limiting cardiovascular autonomic dysfunction in these diseases is orthostatic hypotension, which is particularly prominent in multiple system atrophy. Postprandial hypotension and supine hypertension, as well as dopaminergic therapy, often complicate the management of orthostatic hypotension in patients with parkinsonian syndromes.
DEMENTIA WITH LEWY BODIES
Dementia with Lewy bodies is also known as diffuse Lewy body disease, senile dementia of the Lewy body type, Lewy body variant of Alzheimer disease, and Parkinson disease with dementia.
Dementia with Lewy bodies is descriptive for the entire series of these diseases. Pathologically, it is identical to Parkinson disease with dementia, with the only difference being an objective criterion based on the duration of dementia. Dementia less than 1 year after onset of parkinsonism is considered dementia with Lewy bodies, whereas dementia more than 1 year after the onset of parkinsonism is considered Parkinson disease with dementia. Whether these are separate disorders or two ends of a spectrum of disease is unclear.
Clinical criteria

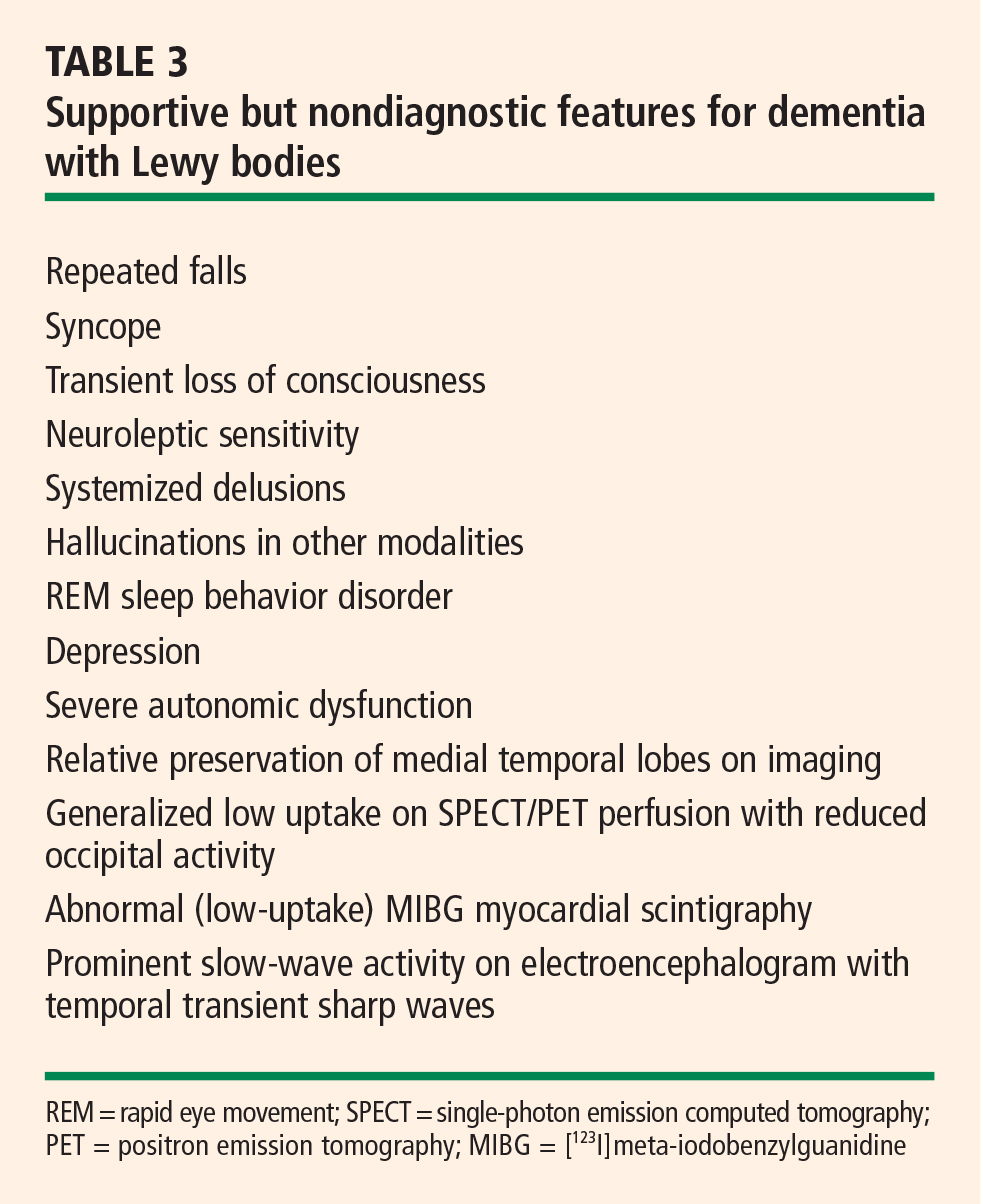
Central feature: progressive cognitive decline. Dementia with Lewy bodies is characterized by prominent progressive cognitive decline that is uncharacteristic of Parkinson disease. In particular, patients with dementia with Lewy bodies have fluctuating cognition, pronounced variations in attention, and early hallucinations when either off medications or on low doses of dopamimetic medications.
Pattern of dementia is more subcortical than cortical. The cognitive changes are different from those present in Alzheimer disease. In contrast to patients with Alzheimer disease, those with dementia with Lewy bodies have more subcortical than cortical dementia, resulting in executive dysfunction and inattention, whereas patients with Alzheimer disease have dysfunction of naming and memory.8
Pathology: diffuse distribution of Lewy bodies. As in Parkinson disease, the pathology is characterized by the appearance of Lewy bodies (positive stain for alpha-synuclein), but their distribution is more diffuse than in Parkinson disease and includes the brainstem, subcortical nuclei, limbic cortex, and neocortex, which may lead to hallucinations in affected patients.
Autonomic features are also diffuse. Autonomic features are also more common in dementia with Lewy bodies than in idiopathic Parkinson disease, which may relate to the different distribution of pathology in these diseases. Significant autonomic failure is present in 62% of patients with dementia with Lewy bodies,9 and the autonomic failure is believed to result from dysfunction of peripheral postganglionic neurons in addition to numerous cortical and brainstem Lewy bodies. Patients with dementia with Lewy bodies also have significant deposits in intermediolateral columns of the spinal cord and autonomic ganglia and sympathetic neurons.
PURE AUTONOMIC FAILURE
The pathology of pure autonomic failure is similar to that of dementia with Lewy bodies and idiopathic Parkinson disease. In contrast to these disorders, however, pure autonomic failure is characterized by a less significant presence of Lewy bodies in the cortex and brainstem, although the pathology in the spinal cord and peripheral nervous system is quite prominent.
Pure autonomic failure is a sporadic disease with onset after age 60 years. It is characterized by slowly progressive isolated impairment of the autonomic nervous system, which manifests particularly as orthostatic hypotension and also as significant bladder and sexual dysfunction. The condition is ultimately disabling as a result of the orthostatic hypotension.
CARDIOVASCULAR AUTONOMIC DYSFUNCTION
Orthostatic hypotension is the most limiting of the cardiovascular autonomic dysfunctions in the neurodegenerative disorders discussed here. Postprandial hypotension is also prevalent in these disorders, as is supine hypertension, which makes successful treatment of cardiovascular autonomic dysfunction difficult.
Orthostatic hypotension is defined as a decrease in systolic blood pressure of at least 20 mm Hg, or a decrease in diastolic blood pressure of at least 10 mm Hg, upon tilting or standing.
In contrast, in normal subjects the initial response upon standing is a pooling of 500 to 1,000 mL of blood and a reduction in venous return and cardiac output. A resultant decrease in blood pressure would occur if not for the baroreceptor reflex, which increases sympathetic tone and decreases vagal parasympathetic tone. Vasopressin is then released from the posterior pituitary, which increases peripheral vascular resistance, venous return, and cardiac output. As a result, the normal response to standing is a modest decrease in systolic blood pressure—ie, by 5 to 10 mm Hg— and an increase in diastolic blood pressure by a similar amount, as well as a compensatory increase in pulse rate of 10 to 25 beats per minute.
Approaches to therapy for orthostatic hypotension
Nonpharmacologic approaches to orthostatic hypotension include raising the head of the patient’s bed by 30 degrees, use of compression stockings, and liberalizing the use of fluids and salt.
Often, however, patients require pharmacologic therapy. Fluorohydrocortisone and midodrine are the primary drugs used for this purpose, but pyrodostigmine also has shown some efficacy in doses of 60 mg or greater in small clinical trials. Less-effective options include nonsteroidal anti-inflammatory drugs, vasopressin analogs, erythropoietin, and caffeine.
Management of postprandial hypotension
Reducing meal size while increasing the frequency of meals and adding caffeine are dietary approaches to treat postprandial hypotension. Somatostatin analogs may be helpful, although data to support their use for this indication are limited.
Treatment of supine hypertension is more difficult
The management of supine hypertension is difficult in patients with neurodegenerative disorders. Supine hypertension is defined as a blood pressure greater than 140/90 mm Hg, but the threshold for concern is uncertain. Most patients with neurodegenerative disorders are plagued more by hypotension than by hypertension, but the hypertension can be deleterious to their health, particularly when they are being treated for their hypotension during the day. Some clinicians choose to treat the hypertension if it is significant in the evening. Most important is to remove the midodrine at night and minimize the use of fluorohydrocortisone. Other options are nitrate derivatives, hydralazine, and calcium channel blockers. The proposed benefits of minoxidil and clonidine are controversial.
Autonomic complications of dopaminergic therapy
Complicating the management of autonomic dysfunction in patients with parkinsonian features is that drug therapies for Parkinson disease exacerbate orthostatic hypotension to varying degrees. Selegiline, amantadine, and dopamine agonists exacerbate orthostasis to a greater degree than levodopa does. Therefore, we are apt to start treatment with levodopa as patients develop more features of autonomic dysfunction, as well as in patients with advanced Parkinson disease or in patients who are older than 70 years of age.
Multiple system atrophy may respond only to high doses of levodopa (> 1 g), and when autonomic symptoms are prominent, patients with multiple system atrophy may not tolerate dopaminergic therapy at all. In patients with dementia with Lewy bodies, the use of dopaminergic therapies is limited not so much by autonomic dysfunction but because of hallucinations and cognitive decline.
SUMMARY
Central autonomic dysfunction predominates in patients with multiple system atrophy. Peripheral autonomic dysfunction predominates in the other parkinsonian disorders with Lewy body pathology, and this includes idiopathic Parkinson disease, dementia with Lewy bodies, and the related disorder, pure autonomic failure, in which there are no parkinsonian features.