Biofeedback: An overview in the context of heart-brain medicine





ABSTRACT
Biofeedback involves the monitoring and use of physiologic information to teach patients to modify specific physiologic functions. Common modalities for biofeedback include surface electromyography, respiration rate and depth, skin surface temperature, cardiovascular reactivity, and electrodermal response. Clinical biofeedback therapy broadly involves either the direct feedback learning model or the therapeutic/stress-management/biofeedback model, which emphasizes the need to understand each patient as an individual. Biofeedback interventions have been deemed efficacious or probably efficacious in treating a number of medical disorders, and are increasingly embraced by the public as well as by health care providers and payors.
LEARNING AND MODELS OF BIOFEEDBACK
Accurate feedback facilitates the learning of any skill, whether it be sinking a golf putt, solving an algebra problem, or controlling physiologic behavior. A man playing darts blindfolded is unlikely to achieve as good a score as he would with the blindfold off, because feedback makes a difference.5
Four conditions are important for effective learning;5 the learner must:
- Have the capacity to respond
- Be motivated to learn
- Be positively reinforced for learning
- Be given accurate information about the results of the learning effort.
Direct feedback learning model
The direct feedback learning model assumes that adding feedback to the other important conditions of learning will result in a patient gaining control of the relevant physiology being targeted. This model has been used in treating many disorders, including Raynaud phenomenon and urinary and fecal incontinence.
Biofeedback training in this model may involve a coach/instructor/therapist only to the extent of explaining the equipment and its use. In other words, the coach “teaches the patient how to use the mirror.” More commonly.particularly for training in lowered arousal for patients in whom stress reactivity is a significant factor in the development and maintenance of excessive (sympathetic nervous system) arousal that leads to symptoms.a skilled therapist is present. The therapist not only teaches the patient how to use information from biofeedback instruments but also guides the patient in identifying and changing cognitive, emotional, and behavioral patterns that contribute to excessive reactivity. The relationship of physiologic reactivity to the subject matter under discussion also helps diagnostically in identifying stressful areas of life, particularly in psychophysiologic responders who are repressive and denying and who are not good at identifying the stressors in their lives. The equipment becomes a mirror that lets the patient see a problem that he or she had not identified as such.5
Therapeutic/stress-management/biofeedback model
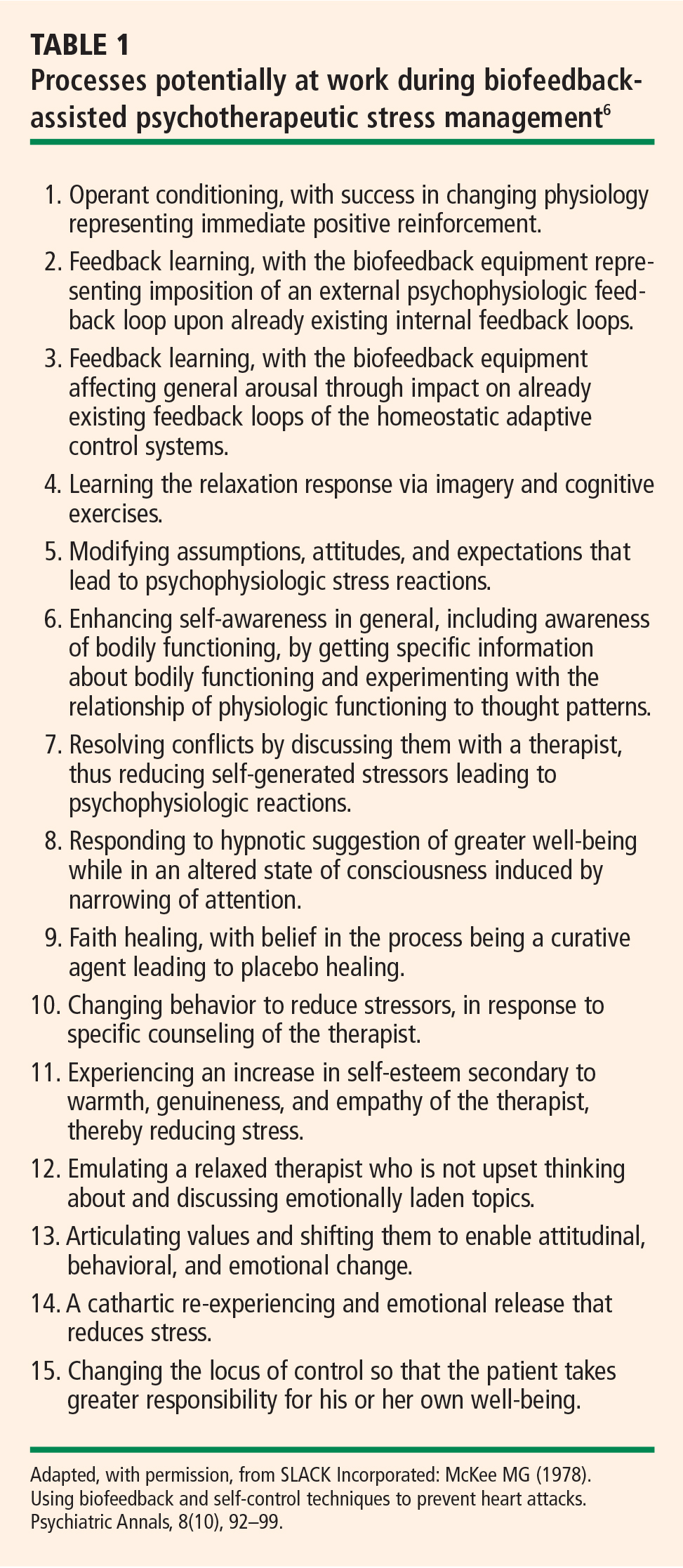
When treating patients with disordered physiology (including autonomic imbalance) in the therapeutic/stress-management/biofeedback model, it is essential to understand each patient as an individual. In this model, stress management and psychotherapeutic interventions address particular vulnerabilities that lead to excessive arousal. This approach starts with a psychophysiologic assessment in which resting levels of relevant physiologic dimensions are measured; this is followed by imposition of stressors to measure reactivity and then by a recovery period in which rate and extent of recovery are measured. An interview and psychological test help determine which cognitive, emotional and behavioral patterns contribute to vulnerability. Patients typically respond well to this approach. It is common for patients to use such descriptions as, “I break out in a cold sweat when I’m stressed,” or “I feel heartsick when I’m stressed,” which suggests that the notion of mind-body interaction resonates with patients.6
CRITERIA FOR EVALUATING EFFICACY OF BIOFEEDBACK INTERVENTIONS
Several years ago a task force of the Association for Applied Psychophysiology and Biofeedback and the Society for Neuronal Regulation published criteria for evaluating the clinical efficacy of biofeedback/psychophysiologic interventions.7 These criteria are detailed below.3,7
Level 1: Not empirically supported
This designation applies to interventions supported only by anecdotal reports and/or case studies in non–peer-reviewed venues (ie, not empirically supported).
Level 2: Possibly efficacious
This applies to interventions supported by at least one study of sufficient statistical power with well-identified outcome measures but which lacked randomized assignment to a control condition internal to the study.
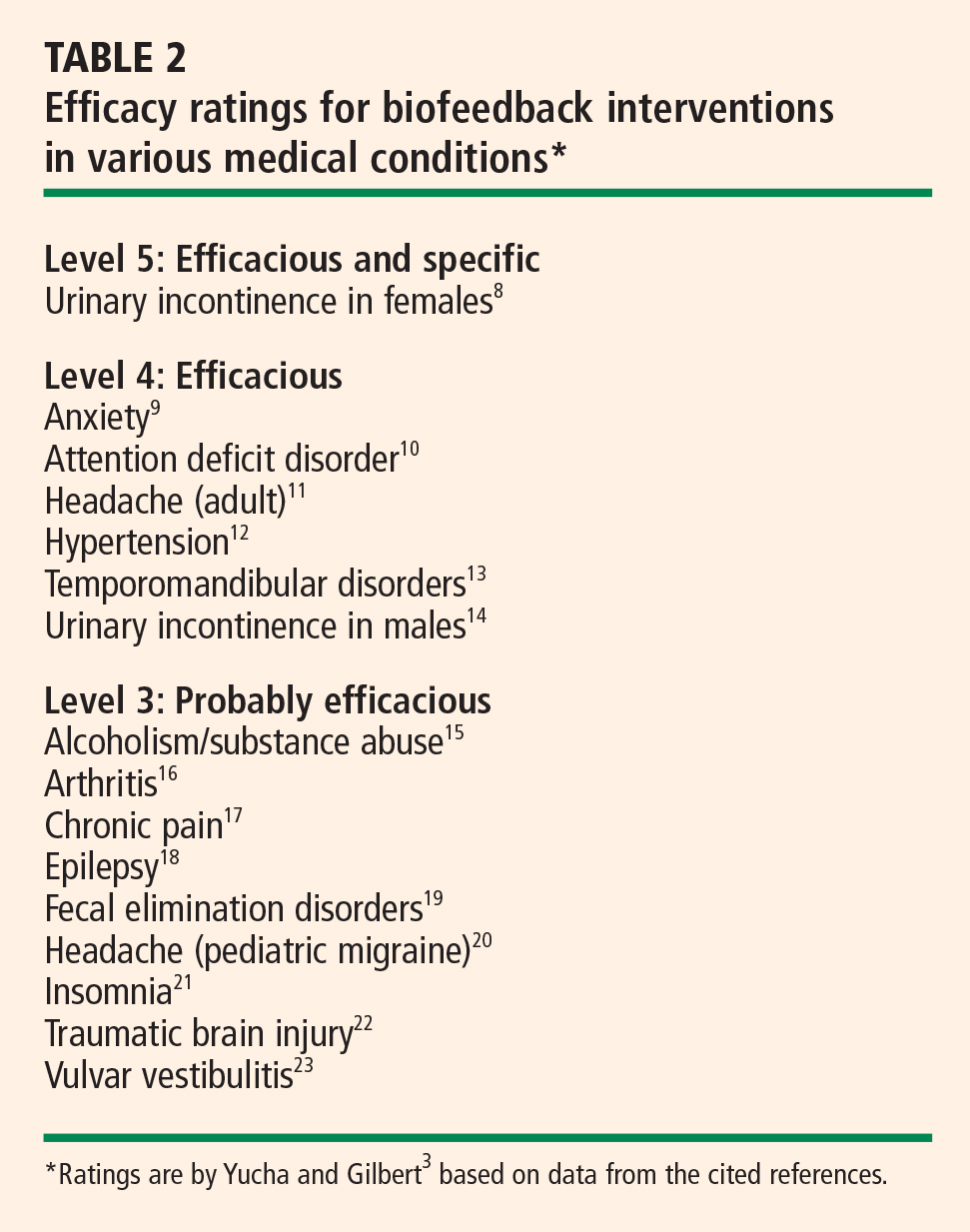
Level 3: Probably efficacious
This applies to interventions supported by multiple observational studies, clinical studies, wait-list–controlled studies, and within-subject and intrasubject replication studies that demonstrate efficacy.
Level 4: Efficacious
a. In a comparison with a no-treatment control group, alternative treatment group, or sham (placebo) control using randomized assignment, the intervention is shown to be statistically significantly superior to the control condition, or the intervention is equivalent to a treatment of established efficacy in a study with sufficient power to detect moderate differences, and
b. The studies have been conducted with a population treated for a specific problem, for whom inclusion criteria are delineated in a reliable, operationally defined manner, and
c. The study used valid and clearly specified outcome measures related to the problem being treated, and
d. The data were subjected to appropriate data analysis, and
e. The diagnostic and treatment variables and procedures were clearly defined in a manner that permits replication of the study by independent researchers, and
f. The superiority or equivalence of the intervention has been shown in at least two independent research settings.
Level 5: Efficacious and specific
This designation applies when the intervention has been shown to be superior to credible sham therapy, pill therapy, or alternative bona fide treatment in at least two independent research settings.
Efficacy ratings for specific disorders
Despite high standards, biofeedback thrives
The above criteria represent high standards. Since biofeedback training is often more like physical therapy or learning a language, double-blind protocols usually are not feasible, nor is sham training. Moreover, the effectiveness of training is perhaps even more difficult to assess in daily practice, with the inevitable multiplicity of confounding variables. Nevertheless, biofeedback training for many disorders is standing the test of both time and outcomes research, and it is increasingly embraced by the public and recognized by health care insurers and professionals alike.