Perioperative medication management: General principles and practical applications





ABSTRACT
An extensive medication history, including the use of nonprescription agents and herbal products, is the foundation of effective perioperative medication management. Decisions about stopping or continuing medications perioperatively should be based on withdrawal potential, the potential for disease progression if therapy is interrupted, the potential for drug interactions with anesthesia, and the patient’s short-term quality of life. In general, medications with withdrawal potential should be continued perioperatively, nonessential medications that increase surgical risk should be discontinued before surgery, and clinical judgment should be exercised in other cases.
KEY POINTS
- Common drugs that have been associated with withdrawal symptoms when discontinued preoperatively include selective serotonin reuptake inhibitors (SSRIs), beta-blockers, clonidine, statins, and corticosteroids.
- In general, most nonsteroidal anti-inflammatory drugs should be stopped at least 3 days before surgery.
- Although ACE inhibitors and angiotensin receptor blockers intensify the hypotensive effects of anesthesia, it may be prudent to continue them perioperatively unless their only indication is for hypertension and the patient’s blood pressure is well controlled.
- Herbal medications should be stopped at least 7 days before surgery, owing to the uncertainly over their actual contents.
- Among psychotropics, SSRIs, tricyclic antidepressants, benzodiazepines, and antipsychotics are generally safe to continue perioperatively.
CASE 3: A PATIENT TAKING HERBAL MEDICATIONS
A 68-year-old woman with a history of hypertension, osteoarthritis, and osteoporosis is scheduled for total hip replacement in 7 days. Her medications include atenolol, hydrochlorothiazide, and alendronate. She also reports taking some natural herbal medications. She does not recall their names initially but calls back with the names: ginkgo biloba for her memory and echinacea for her immune system.
Question: What are your recommendations?
A. Stop all medications now except atenolol and proceed to surgery
B. Stop the herbals now but take all other medications on the morning of surgery
C. Stop the herbals now and take only atenolol on the morning of surgery
D. Continue all medications now and take atenolol and the herbals on the morning of surgery
E. Cancel the surgery and call an herbalist for guidance
The best strategy is to stop the herbals now and tell her to take only atenolol (a beta-blocker) on the morning of surgery.
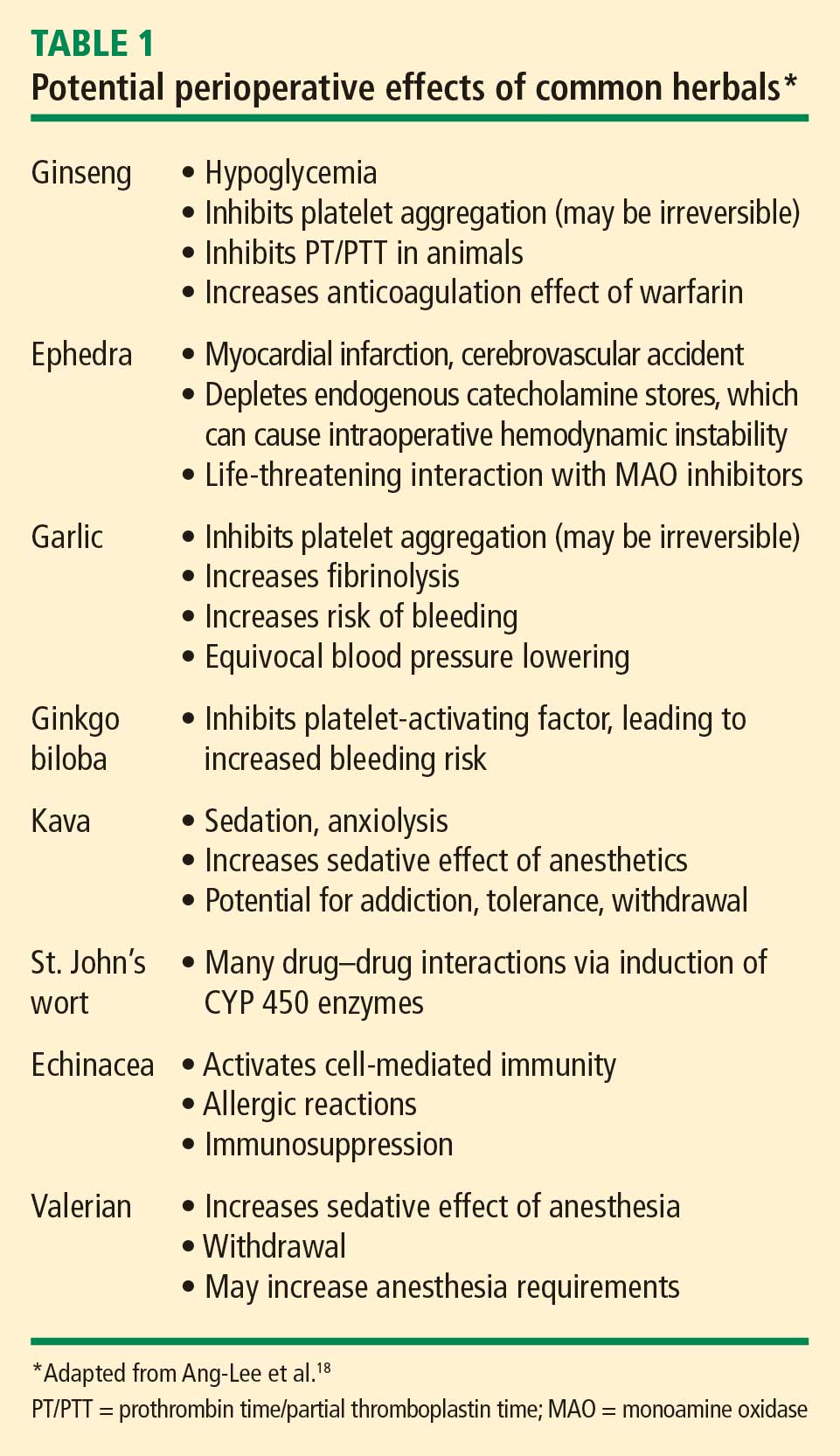
Because the US Food and Drug Administration (FDA) does not regulate herbal products, the contents of these products can vary widely. For example, an analysis using mass spectrometry of 50 commercial ginseng products from 11 countries found that the ginseng content varied from 0% (six preparations) to 9%.19 Catecholamine-type compounds were found in some of the products.19
Because of the uncertainty over their actual contents, herbal medications should be stopped at least 7 days prior to surgery. If a patient is still taking herbal supplements on the day before surgery, I typically alert the anesthesiologist and surgeon.
CASE 4: A PATIENT ON MULTIPLE PSYCHOTROPICS
A 38-year-old woman with a history of severe major depression is scheduled for a mastectomy for breast cancer the next day. Her medications include fluoxetine, lorazepam, and phenelzine, all of which she has been taking for many years.
Question: What is your course of action?
A. Call the surgeon and cancel the surgery
B. Call the surgeon and notify the day-of-surgery anesthesiologist that the patient is taking these agents
C. Stop all the medications now and proceed to the operating room
D. Request a psychiatric consult for an alternative drug regimen
E. Proceed and advise the patient to take all of these agents on the morning of surgery
My approach would be to notify the day-of-surgery anesthesiologist, specifically about the phenelzine, which is a monoamine oxidase (MAO) inhibitor (see below). The other two agents can be taken on the morning of surgery, although fluoxetine has a long half-life, so missing a dose should not be problematic, and lorazepam can be given intravenously if needed.
SSRIs, including fluoxetine, are generally safe perioperatively. Serotonin depletion from platelets, however, increases the risk of bleeding, especially gastrointestinal bleeding, when SSRIs are used with NSAIDs.20–22 A neurosurgical procedure may therefore be especially risky in patients who have not stopped their SSRI if they are also taking an NSAID or an herbal medication that may increase the risk of bleeding. The caveat to stopping SSRIs is the potential for a minor withdrawal syndrome.
Tricyclic antidepressants inhibit the reuptake of norepinephrine and serotonin and may increase the action of sympathomimetics. Although arrhythmias are thought to be a concern with tricyclics, there are no reported cases of association in the literature. In general, I advise continuing triclyclics perioperatively, especially in patients who are on high doses.
Benzodiazepines, including lorazepam, are safe to use perioperatively, and a potential for withdrawal symptoms (hypertension, agitation, delirium, seizures) argues against their discontinuation. Chronic benzodiazepine use may increase anesthetic requirements.
Antipsychotic agents, which include haloperidol, olanzapine, risperidone, and ziprasidone, have multiple routes of administration—intramuscular, oral, sublingual, and intravenous. These agents are generally safe to use in the perioperative period.
MAO inhibitors, including phenelzine, are no longer commonly used and are typically reserved for the treatment of refractory depression. But they merit attention, as their use can cause accumulation of biogenic amines in the central and autonomic nervous systems. There are two types of MAO reactions—excitatory and depressive. Excitatory reactions lead to serotonin syndrome. Depressive reactions induce inhibition of hepatic microsomal enzymes, leading to narcotic accumulation and increased sedation.23
MAO inhibitors are also of concern because of their many drug interactions. When used with indirect sympathomimetics such as ephedrine, they promote a massive release of stored norepinephrine, leading to severe hypertension. When used with opioids like meperidine and dextromethorphan, MAO inhibitors are associated with a serotonin syndrome characterized by agitation, headache, fever, seizures, coma, and death.
Discontinuing MAO inhibitors before the day of surgery is no longer universally recommended, due to the risk of precipitating an exacerbation of major depression. Safe anesthetic regimens in the setting of MAO inhibitors involve avoidance of meperidine (morphine and fentanyl are safe) and use of only direct-acting sympathomimetics.