Prevention of venous thromboembolism after surgery





ABSTRACT
Most surgical patients who require hospitalization are at high risk for venous thromboembolism (VTE) and should receive VTE prophylaxis, usually including pharmacologic prophylaxis. Nevertheless, rates of appropriate perioperative thromboprophylaxis remain stubbornly low, though an expansion in quality-improvement efforts has led to widespread hospital implementation of prophylaxis strategies in recent years. This article reviews important principles and recent developments in perioperative VTE prophylaxis, with a focus on key recommendations and changes in the 2008 update of the American College Chest Physicians’ (ACCP) evidence-based guidelines on antithrombotic therapy.
KEY POINTS
- Effective October 1, 2009, the Centers for Medicare and Medicaid Services is refusing to reimburse for hospital treatment of a primary diagnosis of deep vein thrombosis or pulmonary embolism following recent (within 30 days) hip or knee replacement surgery.
- Mechanical methods of thromboprophylaxis are not effective unless used for at least 18 to 20 hours a day.
- The latest ACCP guidelines recommend extended pharmacologic VTE prophylaxis for up to 28 days in select high-risk patients undergoing general or gynecologic surgery. Extended prophylaxis of varying duration is recommended for patients undergoing major orthopedic procedures.
- Aspirin alone is not recommended for perioperative VTE prophylaxis in any patient group by the ACCP or the International Union of Angiology.
- Patients with renal impairment have fewer anticoagulant options and may require dose adjustment. Weight-based dosing appears to be safe and effective for obese surgical patients.
- New selective and orally administered direct thrombin inhibitors and oral direct factor Xa inhibitors may soon be available for perioperative VTE prophylaxis.
NONPHARMACOLOGIC PROPHYLAXIS STRATEGIES
Does ambulation prevent DVT?
Although it is commonly accepted that walking prevents DVT, this has never been directly tested. Walking may simply be a marker of health, and healthy people are less prone to develop thromboses. We have almost no evidence to show that forcing an unhealthy person to walk helps prevent DVT. Early ambulation offers many benefits and should be encouraged, but it should not be considered DVT prophylaxis; it is simply good hospital care.
Mechanical devices: Adherence is key
Amaragiri and Lees conducted a systematic literature review of randomized controlled trials evaluating the effectiveness of graduated compression stockings (elastic stockings) for preventing DVT in various groups of hospitalized patients.6 The analysis demonstrated a statistically significant reduction in DVT incidence with graduated compression stockings compared with control both among the nine trials in which stockings were used alone (odds ratio = 0.34) and among the seven trials in which stockings were used in addition to another method of thromboprophylaxis (odds ratio = 0.24). Although benefit was demonstrated, many of the trials in this review involved patients undergoing gynecologic surgery and date from the 1970s and 1980s (when obesity was less prevalent), so the applicability of their results today may be limited.
The 8th edition of the ACCP guidelines recommends that mechanical methods of VTE prophylaxis be used primarily in patients who are at high risk of bleeding and that careful attention be directed to ensuring their proper use and optimal adherence.1 The latter point about adherence cannot be emphasized enough, as graduated compression stockings and other mechanical devices have been shown not to be effective unless they are worn at least 18 to 20 hours a day. This degree of adherence is difficult to achieve, as it can severely limit patient mobility and leave patients susceptible to development of pressure ulcers.
Mechanical compression should be initiated prior to induction of anesthesia and continue intraoperatively and then into the postanesthesia care unit. Orders for use of mechanical devices should include instructions in the patient’s medical chart specifying how—and for how many hours per day—they are to be worn. Not doing so leaves the physician vulnerable to litigation, especially as the ACCP guidelines include language on optimal adherence to these devices (“they should be removed for only a short time each day when the patient is actually walking or for bathing”1).
Continuous external compression therapy
Newer mechanical device options include a continuous external compression therapy system that allows patients to be mobile while wearing it and provides rhythmic compression that results in good peak venous flows. Ideally such a device could be put on the patient preoperatively and worn during surgery, throughout the hospital stay, and even at home during recovery. Anecdotally, however, I see patients turn these new devices off at the side of the bed just as often as they do with traditional devices.
Vena caval interruption
Vena caval interruption involves placement of a retrievable vena cava filter before surgery and removal some time later; it offers the potential for VTE prophylaxis in patients who could not tolerate even minor amounts of bleeding, such as certain trauma patients. The Eastern Association for the Surgery of Trauma has put forth a consensus recommendation to consider vena caval interruption in high-risk trauma patients who cannot receive pharmacologic prophylaxis.7 A randomized trial evaluating the usefulness of vena caval interruption for patients undergoing surgery is needed. For now, this intervention should be regarded as experimental and considered only on a highly individualized basis.
PHARMACOLOGIC PROPHYLAXIS
Timing of initiation
Pharmacologic VTE prophylaxis generally should begin 8 to 24 hours postoperatively. Of course, adequate hemostasis is required before initiation, and the net risk/benefit tradeoff with regard to timing of anticoagulant initiation has still not been well studied in many surgical patient populations.
Extended prophylaxis
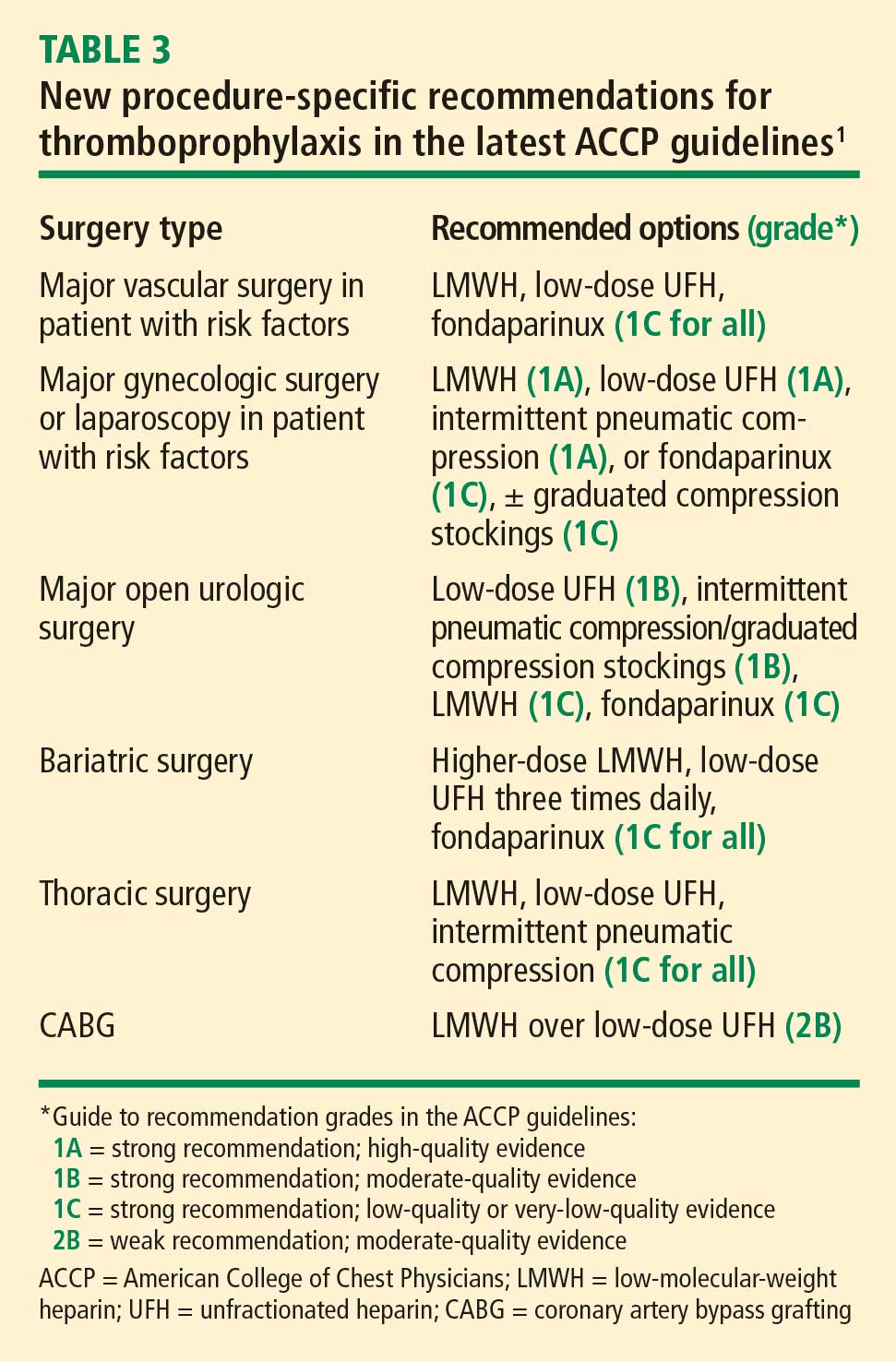
In the update for the 8th edition of its guidelines, the ACCP added an explicit recommendation for extended outpatient prophylaxis with low-molecular-weight heparin (LMWH) for up to 28 days postoperatively in selected high-risk patients undergoing general or gynecologic surgery, including those with cancer or a history of VTE.1 This recommendation was based largely on studies of extended prophylaxis in patients with cancer undergoing colorectal surgery.8
Increased appreciation of the value of extended VTE prophylaxis after discharge is linked to a growing recognition that DVT and PE episodes in the community setting are often related to a recent hospital stay for either medical illness or surgery. A population-based study found that 59% of all community cases of a first lifetime VTE event in residents of Olmsted County, Minn., over a 15-year period could be linked to current or recent (< 30 days) hospitalization or nursing home residence.9 A similar population-based study in the Worcester, Mass., area found that three-fourths of all VTE events in a 3-year period occurred in the outpatient setting.10 Among patients with these outpatient VTE events, a large proportion had undergone surgery (23%) or hospitalization (37%) in the prior 3 months; among those, 67% experienced their VTE within 1 month of their time in the hospital.
These findings are no surprise, since surgery induces a hypercoagulable state that, when combined with individual risk factors such as obesity, old age, or poor heart function, cannot be assumed to return to baseline on postoperative day 4 or 5 just because the patient is being discharged.
Orthopedic surgery
For patients undergoing major orthopedic procedures, the ACCP guidelines recommend against routine screening for VTE with Doppler ultrasonography before discharge if the patient is asymptomatic.1 Such screening is not considered cost-effective because asymptomatic clots often are found, for which treatment is uncertain, and proximal clots may be missed, giving a false sense of security.
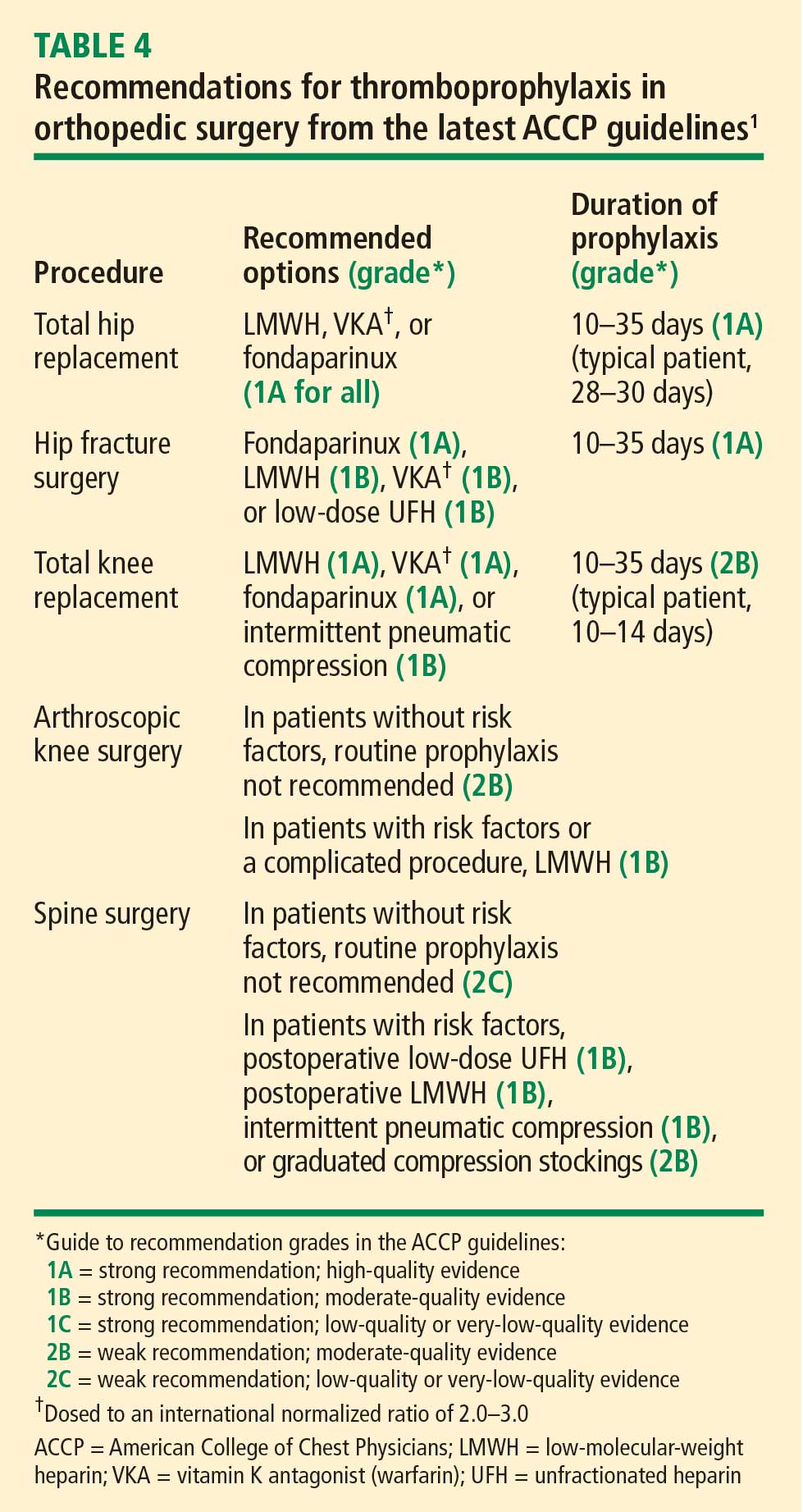
New to the ACCP guidelines in the 8th edition is the recommendation that patients undergoing knee arthroscopy who have risk factors for VTE (or whose procedure is complicated) should receive 1 week of prophylaxis with LMWH.1 Also new are recommendations for patients with risk factors undergoing single- or multilevel laminectomy (Table 4).