Giving anesthesiologists what they want: How to write a useful preoperative consult





ABSTRACT
Anesthesiologists are the primary users of preoperative medical consultations (consults), but the information in consults is often of limited usefulness to anesthesiologists and the rest of the surgical and perioperative team. The purpose of a consult is not to “clear” a patient for surgery but rather to optimize a patient’s underlying disease states before they are compounded by the insult of surgery. Too often consults provide advice on subjects that are in the realm of expertise of the anesthesiologist—such as the type of anesthesia to administer or what intraoperative monitoring to use—and thus risk being ignored. Consults should instead provide specific data about the patient that are pertinent to the surgery, as well as guidance on preoperative and postoperative disease management.
KEY POINTS
- Consults that provide pertinent quantitative data about the patient are helpful—eg, the heart rate at which ischemia was exhibited during stress testing and the degree of ischemia.
- Anesthesiologists do not need assistance with managing intravenous drugs (with the exception of unusual agents), but they can use specific guidance on managing oral medications pre- and postoperatively to best achieve optimization and steady-state concentrations.
- Pertinent recent information (< 5 years old) from the nonanesthesiology literature should be provided.
- Medical consultants should arrange for follow-up care for patients with active conditions not addressed by the surgery.
- Absolute recommendations should be avoided in a consult: the surgical team may have good reason not to follow them, and legal repercussions could ensue. The words “consider” or “strongly consider” usually suffice, except where there is an absolute standard of care.
WHAT ANESTHESIOLOGISTS MAY NOT KNOW―AND NEED FROM CONSULTANTS
How to manage chronic diseases
Follow-up care (eg, for poorly controlled diabetes or hypertension) often can wait until after the operation, and a consultant’s opinion about that is appreciated. It is especially helpful to know that the patient will be followed without the surgeon or anesthesiologist having to arrange for it.
New evidence-based guidance from the literature
One case when recommendations on acute medical management should be provided is when they involve new information from the literature—ie, important data or guidelines published within the prior 5 years or so. It can take time for new information and recommendations to reach all clinicians even within a single specialty. Moreover, important information, such as on the perioperative use of beta-blockers and statins, is not necessarily published in the anesthesiology literature. It is critical to relay information such as the recent recommendation not to withdraw statins prior to surgery, as the current editions of most anesthesiology textbooks have incorrect information suggesting discontinuation. Thus, consultants should include pertinent recent data and guideline recommendations, especially if they go against previous dogma.
Rare diseases, blood disorders, other special cases
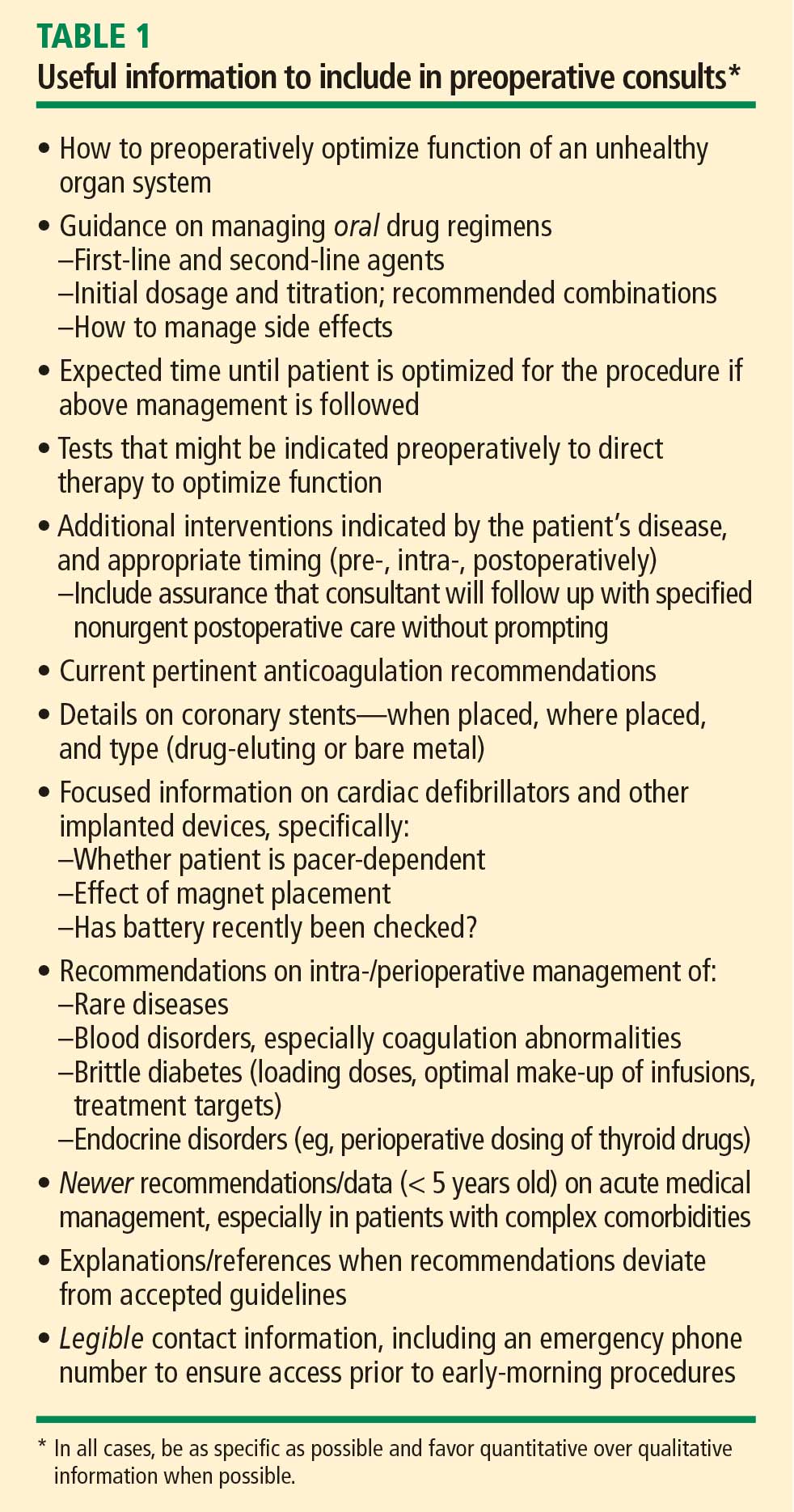
As outlined in Table 1, advice on perioperative management is appreciated for patients with rare diseases, coagulation disorders or other blood disorders, and brittle diabetes and other endocrine disorders, as most anesthesiologists are not intimately familiar with these conditions. Anesthesiologists also need, but often do not get, basic details on coronary stents and other implanted devices (see Table 1), as well as guidance on the latest anticoagulation recommendations, with which it is difficult to keep up to date.
A sensitivity to audience and context
It is always appropriate to ask the surgeon requesting a consult—and the anesthesiologist assigned to the case, if known—what he or she wants to know from the consult. If guidance on specific cases is impractical, it is appropriate to ask the chair of the anesthesiology department, or several anesthesiologists collectively, for general guidance on what they look for from preoperative consults.
Anesthesiologists, like consultants, comprise a broad range of people, and it is always important to be sensitive to context. Generalists who work mainly on healthy patients or in a community setting may have forgotten some of their training in acute medicine and are more likely to appreciate advice on intraoperative care. On the other hand, an anesthesiologist who trained in a cardiothoracic subspecialty fellowship, who routinely deals with issues such as left ventricular assist devices and heart transplants, would not benefit from such advice.
WHAT A CONSULT SHOULD―AND SHOULD NOT―BE
The above advice can be distilled into a few principles:
- A consult is an opportunity for the medical consultant to provide helpful management suggestions to the operative team.
- A fundamental objective of a consult is to optimize a patient’s underlying disease before it is compounded by the insult of surgery.
- The purpose of a consult is never to “clear” a patient for surgery. Whether or not to proceed to surgery is a question for the anesthesiologist, surgeon, and patient to decide after weighing the risks and benefits once the patient’s comorbidities are optimally managed. The consult is an important contributing factor to this decision, but it should never be the mechanism of the decision. Though the note from the surgeon requesting a consult may routinely be written as, “Clear the patient for surgery,” consultants should recognize this for what it is—the surgeon’s attempt to avoid having the anesthesiologist cancel the operation—and refrain from weighing in on “clearance” one way or the other.
CASE STUDY: CARDIAC CONSULT REQUESTED BEFORE FEM-POP BYPASS SURGERY
Cardiovascular problems are the most common reasons for requesting preoperative consults. The following case illustrates a typical scenario for a cardiac consult request and presents examples of good and bad notes requesting consults and good and bad consults written in response.
The case
A 47-year-old man is scheduled for femoral-popliteal bypass surgery. His medical history is significant for diabetes, a myocardial infarction (MI) 3 years ago followed by placement of a stent, and a limited ability to assess exercise tolerance. Evidence of an anteroseptal MI is present on 12-lead electrocardiography. His medications include metoprolol 25 mg twice daily and an oral hypoglycemic agent. His blood pressure is 152/89 mm Hg, heart rate 81 beats per minute, respiratory rate 14 breaths per minute, and arterial oxygen saturation 96% on room air.
The consult request: Bad and good examples
A bad consult request in this case would be, “Clear the patient for surgery.” Although this type of request is routinely written, it is routinely useless.
For this complex surgery with significant fluid requirements, a much better consult request would include several specific requests and questions and might read as follows:
—Please evaluate patient’s post-MI therapy for his CAD. Is further therapy required to optimize CAD treatment?
—Do his blood pressure or diabetic regimens need modification? If so, can this be done postoperatively?
—Please evaluate patient’s myocardial function in light of a lack of info on exercise tolerance. Is an echo indicated?
—Are other tests, therapies, or interventions warranted pre- or postoperatively?
Example of a bad consult
A poorly written consult in a case like this may:
- Include a brief history repeating facts that are already known and noting that “the patient is at his baseline without obvious ischemia.”
- State that the patient is cleared for “spinal” anesthesia. “Clearing a patient for anesthesia” is useless to begin with, but clearing for a certain type of anesthesia places the anesthesiologist in a terrible medicolegal position if general anesthesia turns out to be needed. Moreover, there are no proven major outcome differences related to the type of anesthetic chosen.
- Recommend that “a pulmonary artery catheter might be indicated to monitor hemodynamics.” Besides the fact that such catheters probably do more harm than good, such a recommendation is unnecessary since the anesthesiologist is already expert in managing perioperative care.
- Recommend that “the anesthesia team should monitor the patient carefully in the perioperative arena for hypoxia and hypotension.” Qualitative advice, such as “avoid hypoxia, hypotension, and tachycardia,” is not useful, but quantitative information, such as “during ischemic stress testing, the patient exhibited ischemia when his heart rate went to 142,” can be very helpful.
- State that the patient be sent to the ICU following surgery. Mandating an ICU stay in advance makes no sense unless the operation itself demands ICU care, which is the call of the surgeon and anesthesiologist anyway.
A consult like this doesn’t tell the perioperative team anything that it didn’t already know. Such a consult not only is unhelpful but also actually creates more work since much of the advice needs to be “undone” lest a lawyer see the chart and it not be clear why the consultant’s recommendations were not followed.
Example of a good consult
In contrast, a good consult for this case would involve:
- A detailed history examining the potential for silent ischemia associated with the diabetes, as well as the relationship of the hypertension and beta-blocker therapy to episodes of ischemia. The level of ischemia should be clearly categorized. If it cannot be determined, this should be noted; if it can be determined only that the ischemia is not New York Heart Association class III or IV, note this as well (the perioperative outcomes literature suggests that no preoperative ischemia testing is needed with class I or II angina).
- Guidance on blood pressure optimization in light of the relative urgency of the procedure. Blood pressure need not be normalized preoperatively in this case, but if the operation were totally elective and the consultant felt it could make a difference, it would be appropriate to suggest that blood pressure be optimized beforehand.
- A recommendation on whether and when to change the beta-blocker dosage. If the dosage needs to be increased, the anesthesiologist will want to know how many doses are needed to reach a new steady state. Joint guidelines from the American College of Cardiology (ACC) and American Heart Association (AHA)2 recommend 7 to 30 days, but this time frame is unrealistic in this setting, so more practical advice would be appreciated. A good consult notes any deviation from established guidelines, however, and explains the rationale for such deviation.
- Evaluation of the myocardium at risk. This is especially important with left main disease, as it influences the decision whether to test or intervene versus proceeding with careful beta-blocker titration.
- Evaluation of myocardial function and, if appropriate, a therapy suggestion for optimization.
- Notation of the heart rate or blood pressure thresholds at which ischemia develops if a stress test is performed.