Maternal asthma: Management strategies





ABSTRACT
Asthma in pregnancy is common, and its prevalence is rising. Internists need to be aware of the effects of maternal asthma control on the health of the expectant mother and the baby. With the ever-present worry about medication use and teratogenicity in pregnant women, these patients are often undertreated for their asthma. This review focuses on effects of uncontrolled maternal asthma as well as appropriate management of maternal asthma in the outpatient setting and during exacerbations.
KEY POINTS
- The benefits of good adherence to asthma regimens during pregnancy outweigh the risks associated with the medications used.
- For treatment of reflux disease in pregnant women with asthma, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
- Uncontrolled maternal asthma contributes to poor maternal and fetal outcomes. Management by a multi-disciplinary team, including internist, obstetrician, pharmacist, nurse, allergist, and pulmonologist, improves care and outcomes.
Avoiding triggers
Patients should be advised to avoid asthma triggers such as pet dander, dust mites, pollen, smoke, mold, and perfumes, as this can decrease symptoms and allow for use of lower doses of medications.12 Additionally, smoking cessation must be strongly encouraged, not only to control maternal asthma, but also to prevent harm to the fetus.
MANAGEMENT OF SPECIFIC TRIGGERS
GERD
Reflux disease often worsens during pregnancy, and it can coexist with asthma and can also exacerbate it.14 Optimal control of GERD helps maintain adequate asthma control. For mild reflux symptoms, lifestyle modifications such as elevating the head of bed, avoiding eating too close to bedtime, and avoiding foods that cause heartburn may be adequate.15,16 If medications are needed, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before using a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
Allergic rhinitis
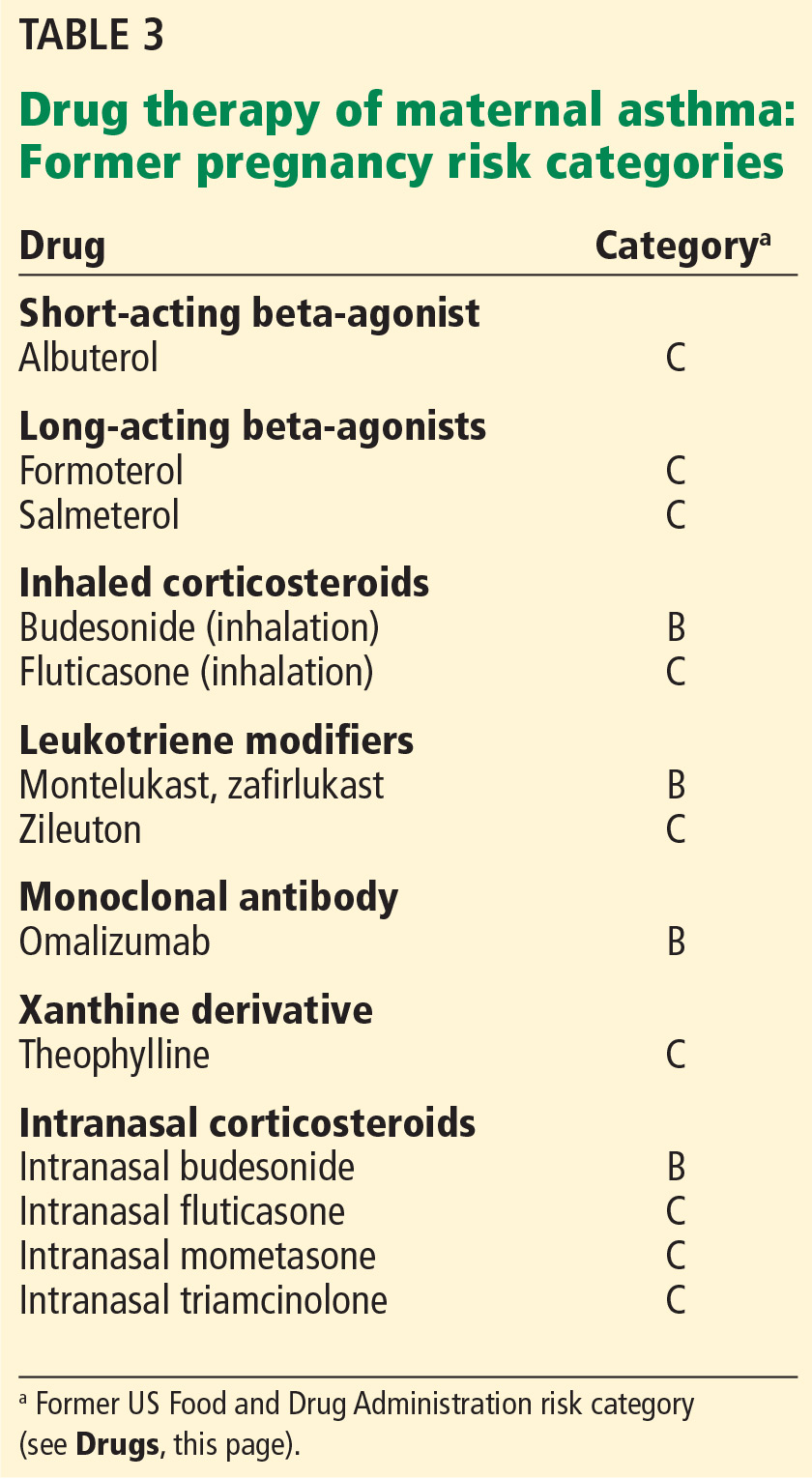
Intranasal corticosteroids are effective against allergic rhinitis in pregnancy (Table 3).12 Montelukast, a leukotriene receptor antagonist, can be used, but data to support its use for allergic rhinitis in pregnancy are limited.
Among antihistamines, second-generation drugs such as cetirizine or loratadine can be considered.12 Oral decongestants such as pseudoephedrine in early pregnancy are associated with a rare congenital fetal abnormality called gastroschisis, caused by vascular disruption.17 Hence, if a nasal decongestant is required in early pregnancy, a local therapy such as an intranasal corticosteroid, short-term oxymetazoline, or an external nasal dilator may be considered.12 These therapies must be combined with avoidance of allergens whenever possible.
Allergies
Diagnostic allergy and skin tests during pregnancy pose a risk of anaphylaxis and thus should be avoided. Instead, the focus should be on obtaining a thorough medical history about exposures and eliminating specific asthma triggers. It is also inadvisable to start allergen immunotherapy during pregnancy because of the risk of anaphylaxis and the effect of treatment on the mother and fetus.18 However, maintenance doses of allergen immunotherapy can be continued during pregnancy.18
Patient education
Because of concern about the risks of taking medications during pregnancy, many women with asthma stop using their inhalers during pregnancy, thus compromising asthma control.8,13 The physician and multidisciplinary team must use every opportunity to emphasize the importance of good asthma control during pregnancy. Inhaler technique should also be reviewed and, if defective, corrected. Again, trigger avoidance and tobacco cessation should be addressed.
Drugs
The NAEPP recommendations state that asthma therapy should be continued during pregnancy, as it is safer both for mother and fetus to avoid exacerbations and uncontrolled asthma.12 Despite this, 25% of primary care physicians instruct their patients to decrease or discontinue their inhaled corticosteroid during pregnancy.19 As with asthma in general, treatment should involve using the lowest dose of drugs that achieves adequate control of symptoms.
In 2015, the US Food and Drug Administration (FDA) amended the labeling rule for medications used in pregnancy and lactation. The previous risk categories A (safest), B, C, D, and X (highest risk) are in the process of being removed from labels for all human prescription drugs and biologic products, to be replaced with a summary of the risks of taking the drug during pregnancy and lactation, a discussion of the data supporting the use, and relevant information to help healthcare providers make prescribing decisions and counsel women about the use of drugs during pregnancy and lactation (www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/Labeling/ucm093307.htm).