Treating Helicobacter pylori effectively while minimizing misuse of antibiotics





ABSTRACT
Experts now recommend that all Helicobacter pylori infections be eradicated unless there are compelling reasons not to. As with other infectious diseases, effective therapy should be based on susceptibility.
KEY POINTS
- We recommend clinicians have 2 first-line options to accommodate prior antibiotic use or drug allergy.
- We recommend 4-drug combinations as first-line treatments, ie, either concomitant therapy or bismuth-containing quadruple therapy, to be taken for 14 days.
- Concomitant therapy consists of the combination of amoxicillin, metronidazole, clarithromycin, and a proton pump inhibitor.
- Bismuth quadruple therapy consists of the combination of bismuth, tetracycline, metronidazole, and a proton pump inhibitor.
- After 2 treatments have failed, therapy with different regimens should be based on susceptibility testing.
Need for 14 days of therapy
H pylori occupies a number of different niches in the body ranging from gastric mucus (which is technically outside the body) to inside gastric epithelial cells. As a general rule, 14-day therapy provides the best results, in part because the longer duration helps kill the organisms that persist in different niches.14,15
In addition, proton pump inhibitors, which are part of all the currently recommended regimens, require 3 or more days to reach their full antisecretory effectiveness, which further limits the effectiveness of short-duration therapies.
Shorter regimens should be used only if they are proved to be as good as 14-day regimens and if both achieve 95% or greater cure rates with susceptible infections.
How to choose a therapy
Since rational infectious-disease therapy is based on susceptibility, one should start by considering the susceptibility pattern in the local population and, therefore, the likely susceptibility in the patient in front of us.
Unfortunately, we do not yet have local or regional susceptibility data on H pylori for most locales. Until those data are available, we must use the indirect information that is available, such as the patient’s history of antibiotic use.
Triple therapy should not be used empirically
Triple therapy (Table 1) consists of the combination of:
- Clarithromycin or metronidazole or a fluoroquinolone
- Amoxicillin
- A proton pump inhibitor.
However, prior use of a macrolide (eg, erythromycin, clarithromycin, or azithromycin), metronidazole, or a fluoroquinolone (eg, ciprofloxacin, levofloxacin) almost guarantees resistance to those drugs. In the United States, resistance to clarithromycin, metronidazole, levofloxacin, and related drugs is already widespread, and none should be used empirically in triple therapies. In contrast, amoxicillin, tetracycline, and furazolidone can often be used again, as resistance to them is rare even with prior use.
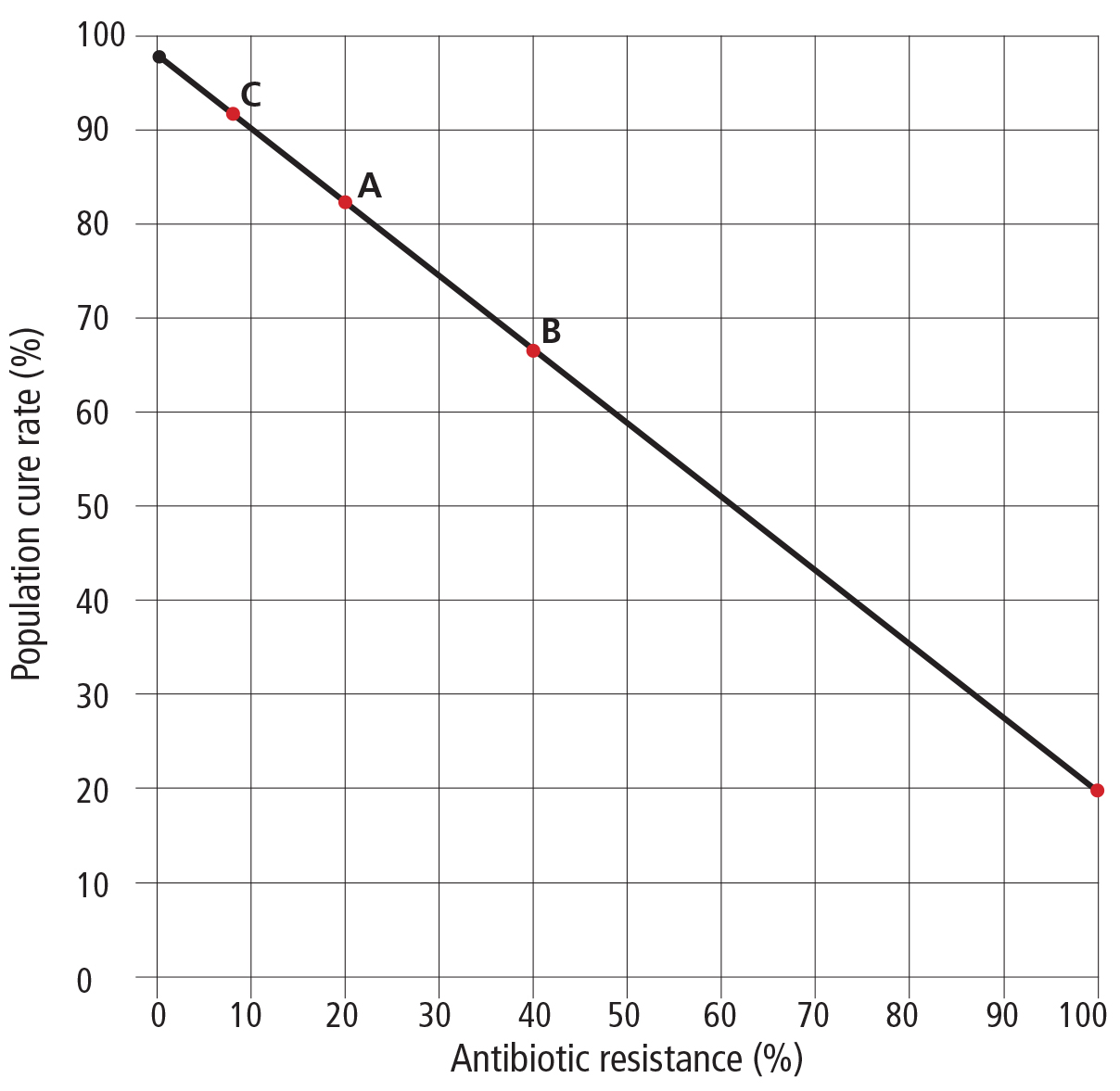
For example, 14 days of clarithromycin triple therapy (clarithromycin, amoxicillin, and a proton pump inhibitor) can be expected to cure more than 95% of patients who have susceptible infections and about 20% of those with resistant infections.16 This 20% is due to the proton pump inhibitor and amoxicillin, as the contribution to the cure rate from clarithromycin is close to zero.
If the prevalence of resistance to clarithromycin is 25%, the cure rate in the entire population will be a little more than 75%—97% in the 75% of the population with susceptible infections and 20% in patients who previously received clarithromycin (Figure 1).
If we know that our patient has an infection that is susceptible to clarithromycin, metronidazole, or levofloxacin, good results could be achieved with triple therapy that includes a proton pump inhibitor, for 14 days. Fluoroquinolones have a number of black-box warnings from the US Food and Drug Administration (www.fda.gov/Drugs/DrugSafety/ucm500143.htm) and should always be a last choice. However, in the United States, lacking definite data about susceptibility to clarithromycin, metronidazole, and levofloxacin, we should assume resistance is present and use a 4-drug regimen (eg, concomitant therapy or bismuth quadruple therapy).
Concomitant therapy is preferred
Concomitant therapy is the combination of:
- Amoxicillin
- Metronidazole
- Clarithromycin
- A proton pump inhibitor.
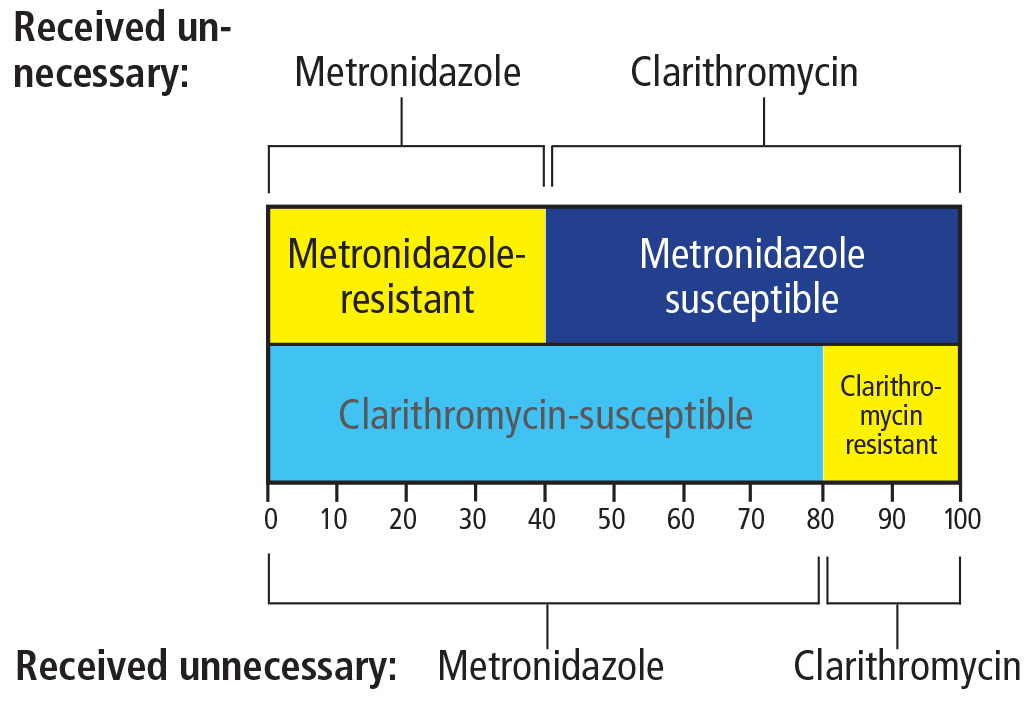
Functionally, this is a combination of clarithromycin and metronidazole triple therapies, given simultaneously.17 The premise is that even though the prevalence of metronidazole resistance in the United States is high (20%–40%), and so is the prevalence of clarithromycin resistance (about 20%), the prevalence of resistance to both drugs at the same time is expected to be low (eg, 0.4 × 0.2 = 0.08, or 8%) unless the drugs had previously been used together, as in some older regimens that contained both. Thus, the metronidazole will kill the clarithromycin-resistant but metronidazole-susceptible strains, and the clarithromycin will kill the clarithromycin-susceptible, metronidazole-resistant strains. Only with dual resistant strains will this regimen fail (with a 20% cure rate due to the proton pump inhibitor and amoxicillin and a population cure rate of slightly more than 90%).
The downside of this highly recommended therapy is that all who receive it are getting an antibiotic that they don’t need, which is, in a global sense, inappropriate. In other words, all those who are cured by clarithromycin also receive metronidazole, which plays no role in treatment success, and those cured by metronidazole receive unneeded clarithromycin (Figure 2). Had susceptibility testing been available, those with susceptible strains would have received appropriate triple therapies, and those with dual resistance would not have received either antibiotic.
Thus, while we recommend concomitant therapy as an empiric regimen in populations that do not have high levels of resistance to metronidazole or clarithromycin (as those would also have a high prevalence of dual resistance), one must be aware of the “dirty little secret” of inappropriate antibiotic use that accompanies it and some other H pylori therapies (eg, vonoprazan triple therapy in Japan).18–20