Participatory pharmacotherapy: 10 strategies for enhancing adherence





Engaging patients as partners in treatment can improve outcomes.
Psychiatric patients stand to benefit greatly from adhering to prescribed pharmacotherapy, but many patients typically do not follow their medication regimens.1,2 Three months after pharmacotherapy is initiated, approximately 50% of patients with major depressive disorder (MDD) do not take their prescribed antidepressants.3 Adherence rates in patients with schizophrenia range from 50% to 60%, and patients with bipolar disorder have adherence rates as low as 35%.4-6 One possible explanation for “treatment-resistant” depression, schizophrenia, and bipolar disorder may simply be nonadherence to prescribed pharmacotherapy.
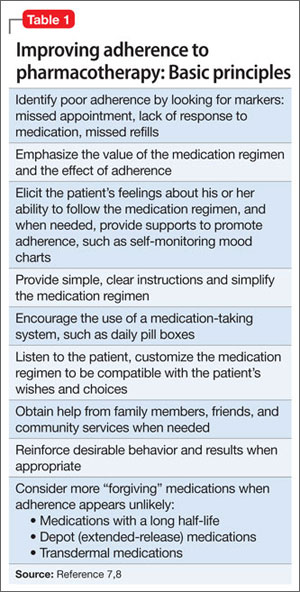
Several strategies have been used to address this vexing problem (Table 1).7,8 They include individual and family psychoeducation,9,10 cognitive-behavioral therapy,11 interpersonal and social rhythm therapy, and family-focused therapy. This article describes an additional strategy I call “participatory pharmacotherapy.” In this model, the patient becomes a partner in the process of treatment choices and decision-making. This encourages patients to provide their own opinions and points of view regarding medication use. The prescribing clinician makes the patient feel that he or she has been listened to and understood. This and other techniques emphasize forming a therapeutic alliance with the patient before initiating pharmacotherapy. The patient provides information on his or her family history, medical and psychiatric history, and experience with previous medications, with a specific focus on which medications worked best for the patient and family members diagnosed with a similar condition.
Getting patients to participate
One of the fundamental tasks is to encourage patients to accept a participatory role, determine their underlying diagnosis, and co-create a treatment plan that will be most compatible with their illness and their personality. There are 10 components of establishing and practicing participatory pharmacotherapy.
1. Encourage patients to share their opinion of what a desirable treatment outcome should be. Some patients have unrealistic expectations about what medications can achieve. Clarify with patients what would be a realistic expectation of pharmacotherapy, and modify the patient’s beliefs to be compatible with a more probable outcome. For example, Ms. D, a 46-year-old mother of 2, is diagnosed with MDD, recurrent type without psychotic features. She states she expects pharmacotherapy will alleviate all symptoms and allow her to achieve a new healthy, happy state in which she will be able to laugh, socialize, and have fun every day for the rest of her life. Although achieving remission is a realistic and desirable treatment goal, Ms. D’s expectations are idealistic. Helping Ms. D accept and agree to realistic and achievable outcomes will improve her adherence to prescribed medications.
2. Encourage patients to share their ideas of how a desirable outcome can be accomplished. Similar to their expectations of outcomes, some patients have an unrealistic understanding of how treatment is conducted. Some patients expect treatment to be limited to prescribed medications or a one-time injection of a curative drug. Others prefer to use herbs and supplements and want to avoid prescribed medications. Understanding the patient’s expectations of how treatment is carried out will allow clinicians to provide patients with a rational view of treatment and establish a partnership based on realistic expectations.
3. Engage patients in choosing the best medication for them. Many patients have preconceived ideas about medications and which medicine would be best for them. They get this information from various sources, including family members and friends who benefitted from a specific drug, personal experience with medications, and exposure to drug advertising.
Understanding the patient’s preference for a specific medication and why he or she made such a choice is critical because doing so can take advantage of the patient’s self-fulfilling prophecies and improve the chances of obtaining a better outcome. For example, Mr. O, a 52-year-old father of 3, has been experiencing recurrent episodes of severe panic attacks. His clinician asked him to describe medications that in his opinion were most helpful in the past. He said he preferred clonazepam because it had helped him control the panic attacks and had minimal side effects, but he discontinued it after a previous psychotherapist told him he would become addicted to it. Obtaining this information was valuable because the clinician was able to clarify guidelines for clonazepam use without the risk of dependence. Mr. O is prescribed clonazepam, which he takes consistently and responds to excellently.
4. Involve patients in setting treatment goals and targeting symptoms to be relieved. Actively listen when patients describe their symptoms, discomforts, and past experiences with treatments. I invite patients to speak uninterrupted for 5 to 10 minutes, even if they talk about issues that seem irrelevant. I then summarize the patient’s major points and ask, “And what else?” After he or she says, “That’s it,” I ask the patient to assign a priority to alleviating each symptom.