The Impact of COVID-19 on Colorectal Cancer Screening Programs






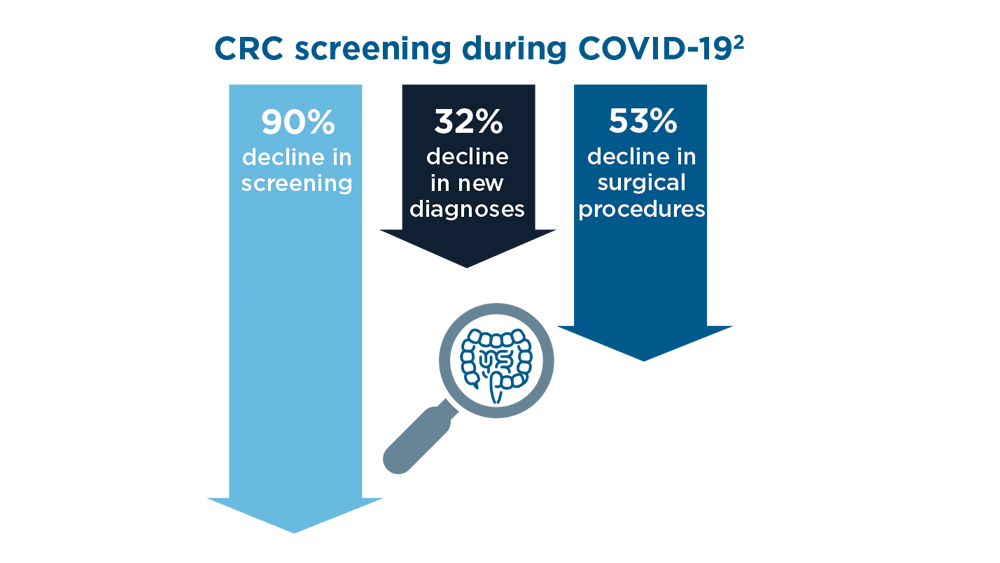
Even before the pandemic, CRC screening was underutilized, despite clear evidence that CRC screening by colonoscopy and stool-based tests was cost-effective and saved lives.1 On March 18, 2020, national agencies and health organizations made necessary initial recommendations to delay nonurgent surgeries and medical procedures, thus causing unprecedented disruptions in CRC screening.2 These delays also risked exacerbating persistent racial and ethnic disparities in CRC screening and outcomes, which had been narrowing.3
COVID-19’s impact on CRC screening was not a singular event. Members of racial and ethnic minority groups, those with limited income, and other historically medically underserved populations were inordinately affected by the disease itself. These populations had the greatest morbidity and mortality from COVID-19,4 and they were understandably more reluctant to return to care,5 including CRC screening.
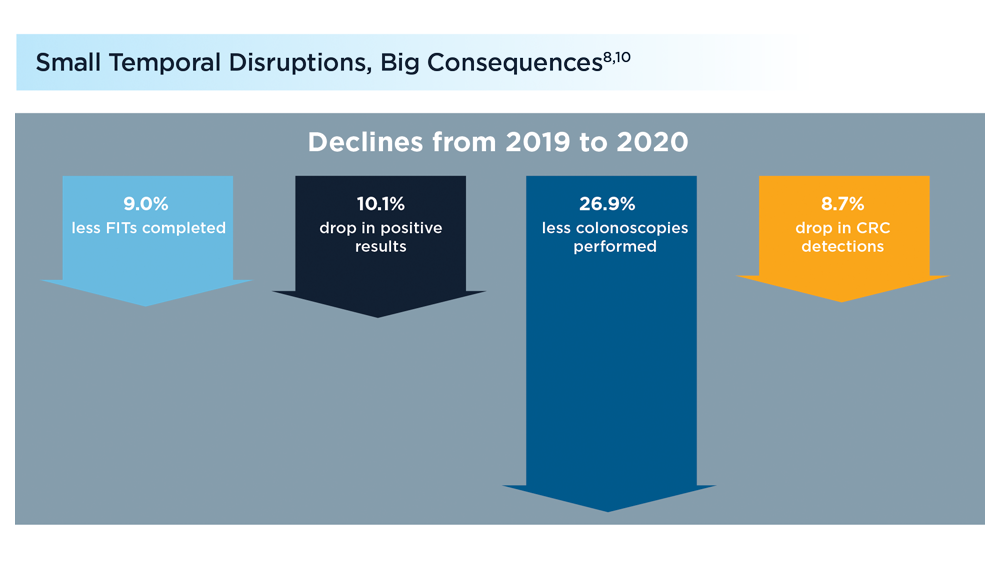
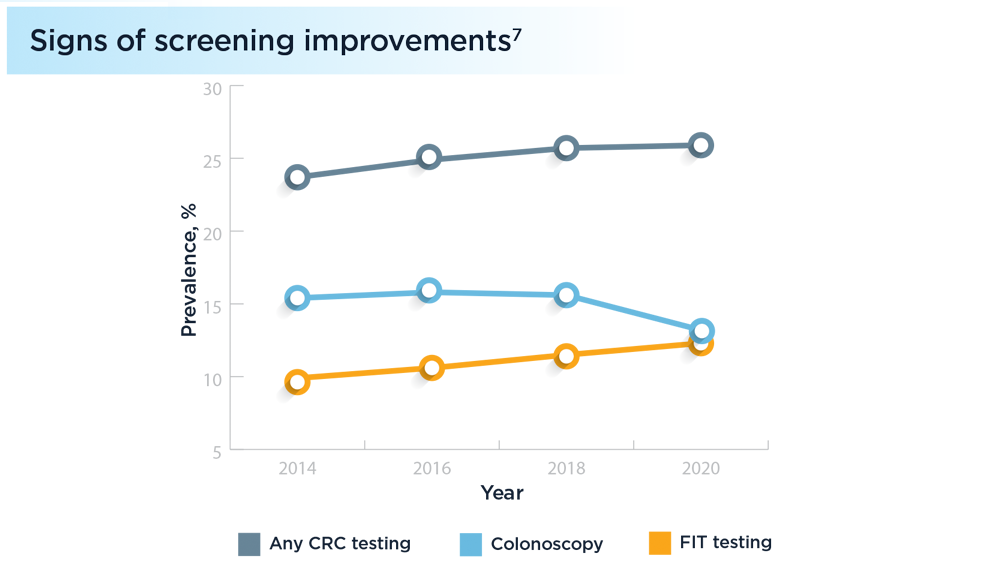
Since the onset of the pandemic, at home stool-based tests, including FIT, have emerged as promising alternatives for CRC screening due to low cost, ease of completion, and preference in low-resourced settings where CRC mortality is high.6,7 In an integrated health system, a FIT-based CRC screening program increased screening participation8 and nearly eliminated Black-White mortality differences over a 10-year period.9 Yet, COVID-19 demonstrated that even small disruptions in such organized programs could have substantial consequences in detecting and preventing CRC.10
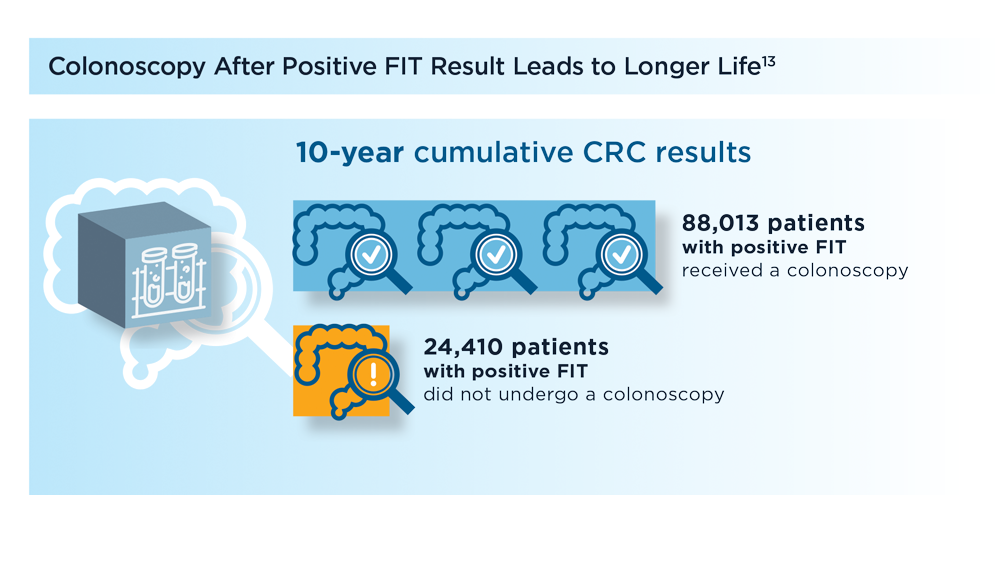
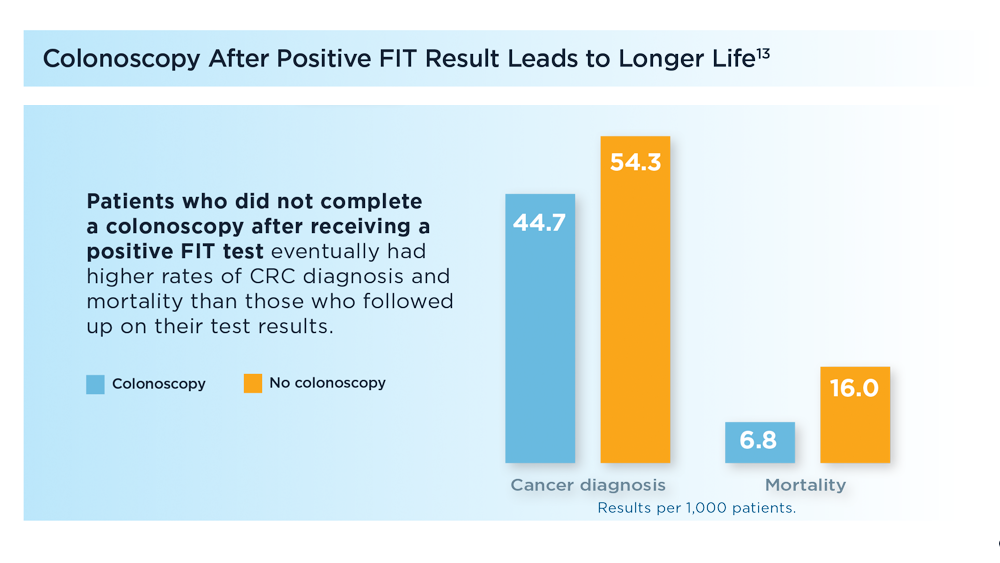
Mailed-to-the-home, stool-based CRC screening tests, including FIT, offer promise for increasing screening rates,11 but must be implemented as part of a broader CRC screening program to realize maximal benefit.12 For example, to ensure that mailed FIT programs do not exacerbate racial and ethnic disparities in CRC outcomes, abnormal results must be followed by a colonoscopy.13 Thankfully, gastroenterology societies including the American Gastroenterological Association, in partnership with federal agencies and advocacy organizations, are leading the way by providing models that can improve screening and follow-up of abnormal results.14
The COVID-19 pandemic has provided our specialty with a clear mandate: To develop long-term solutions that lead to consistent, effective, and trustworthy care for groups who have been historically medically underserved. CRC screening is a valuable way to accomplish this goal.3,15 Doing so is critical for 2 reasons: (1) to maintain momentum in addressing persistent health care disparities, and (2) to guide efforts toward achieving health equity where gaps in care remain.