Travelers’ Diarrhea: Prevention, Treatment, and Posttrip Evaluation





TREATING TD AND ASSOCIATED SYMPTOMS
Antibiotic treatment
Given that most cases of TD are caused by bacterial pathogens, antibiotics are considered the mainstay of treatment. Concerns about the ill effects of antibiotic use in the case of enterohemorrhagic E coli (EHEC O157:H7) can be allayed because this strain is rarely a cause of TD.9
Consider local resistance patterns and risk for invasive infection. Which antibiotic to recommend is governed by the antibiotic resistance patterns prevalent in the travel destinations and by the risk for infection by invasive pathogens. Invasive TD is generally caused by Campylobacter, Shigella, or Salmonella and manifests clinically with bloody diarrhea, fever, or both. Rifaximin at a dose of 200 mg orally three times daily is effective for noninvasive TD.31,32
However, travelers who develop invasive TD need an alternative to rifaximin. (Those who advocate reserving antibiotic treatment only for invasive diarrhea will not see a role for rifaximin in the first place.) In most invasive cases, a fluoroquinolone will suffice.10-12,19,32 However, increasing prevalence of fluoroquinolone-resistant Campylobacter species has been reported in South and Southeast Asia. In those locations, azithromycin is an effective alternative, albeit with risk for nausea.33
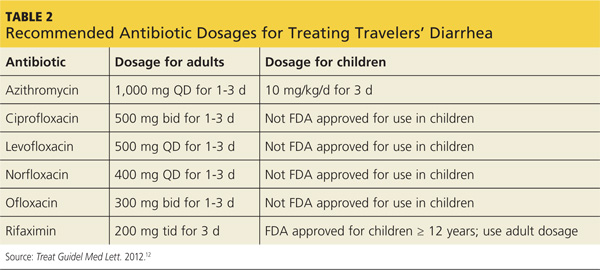
Table 2 provides details of recommended antibiotic dosages for adults and children. The duration of treatment is generally one day unless symptoms persist, in which case a three-day course is recommended.10-12,19,32 If the traveler experiences persistent, new, or worsening symptoms beyond this point, immediate evaluation by a clinician is required.
Nonantibiotic treatment
The antimotility agent loperamide is well established as an antidiarrheal agent. Its effective and safe use as an adjunct to antibiotics in the treatment of TD has been demonstrated in several studies.10-12,19,32,34 It is generally not used to treat children with TD.9
No other nonantibiotic treatment for TD has significant guideline or clinical trial support. Bismuth subsalicylate can be helpful in treating TD,35 but it is not often recommended because of the aforementioned adherence difficulties and because antibiotics and loperamide are effective.
Oral rehydration is usually a mainstay of treating gastrointestinal disease among infants and children. However, it, too, has a limited role in cases of TD, because dehydration is not usually a significant part of the clinical presentation—perhaps because vomiting is not often prominent.
Advice regarding safe food and beverage choices is essential for the patient and her children. Despite the increased risk for TD due to her history and her use of the immunosuppressant methotrexate, she decides not to pursue antibiotic prophylaxis. Bismuth is also contraindicated because of the methotrexate. Her teenage daughter declines bismuth prophylaxis, and her toddler is too young for it.
The patient does accept a prescription for azithromycin for herself and her daughters, in case they experience TD. This choice is appropriate given the destination of India and concern about Campylobacter resistance to fluoroquinolones. You also recommend loperamide for use by the mother and older child, in conjunction with the antibiotic.
Two weeks after their trip abroad, the travelers return for an office visit. On the trip, the mother and toddler experienced diarrhea, which responded well to your recommended management. The older child was well during the trip, but she developed diarrhea, abdominal pain, and anorexia one week after returning to the US. These symptoms have persisted despite a three-day course of azithromycin and loperamide.
Continued on next page >>