Clostridium difficile–Associated Diarrhea and Colitis: A Significant Cause of Nosocomial Infection





Infection with C. difficile may produce a wide range of clinical manifestations, including asymptomatic carriage, mild-to-moderate diarrhea, and fulminant disease with pseudomembranous colitis (10). In patients who develop CDAD, symptoms usually begin soon after colonization. Colonization may occur during antibiotic treatment or up to several weeks after a course of antibiotics. CDAD typically is associated with the passage of frequent, loose bowel movements consistent with proctocolitis. Mucus or occult blood may be present, but visible blood is rare.
Diagnosis
The diagnosis of CDAD is based on a history of recent or current antibiotic therapy, development of diarrhea or other evidence of acute colitis, and demonstration of infection by toxigenic C. difficile, usually by detection of toxin A or toxin B in stool sample.
Practical Guidelines for Diagnosis of C. difficile Diarrheal Syndromes
- The diagnosis should be suspected in anyone with diarrhea who has received antibiotics within the previous 2 months and/or whose diarrhea begins 72 hours or more after hospitalization.
- When the diagnosis is suspected, a single stool specimen should be sent to the laboratory for testing for the presence of C. difficile and/or its toxins.
- When diarrhea persists despite a negative stool toxin result, one or two additional samples may be sent for testing with the same or different tests (4). Endoscopy is reserved for special situations, such as when a rapid diagnosis is needed and test results are delayed or the test is not highly sensitive, when the patient has ileus and stool is not available, or when other colonic diseases are also a consideration.
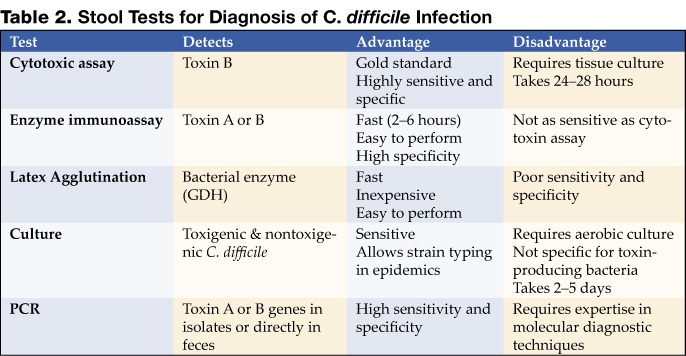
There is as yet no simple, inexpensive, rapid, sensitive and specific test for diagnosing C. difficile diarrhea and colitis, nor are all the available tests suitable for adoption by every laboratory (Table 2) (11).
Endoscopic Diagnosis of C. difficile Diarrhea and Colitis
Sigmoidoscopy and colonoscopy are not indicated for most patients with CDAD (10,12). Endoscopy is helpful, however, in special situations, such as when the diagnosis is in doubt or the clinical situation demands rapid diagnosis. The results of endoscopic examination may be normal in patients with mild diarrhea or may show nonspecific colitis in moderate cases. The finding of colonic pseudomembranes in a patient with antibiotic-associated diarrhea is virtually pathognomonic for C. difficile colitis. A few patients without any diagnostic features in the rectosigmoid have pseudomembranes in the more proximal areas of the colon (13). Other endoscopic findings include erythema, edema, friability, and nonspecific colitis with small ulcerations or erosions.