Binge-Eating Disorder: Prevalence, Predictors, and Management in the Primary Care Setting





From the Department of Psychology, Eastern Michigan University, Ypsilanti, MI.
Abstract
- Objective: To describe the epidemiology, clinical features, clinical course, medical complications, and treatment of binge-eating disorder (BED).
- Methods: Review of the literature.
- Results: BED, the most common eating disorder, is a distinct pattern of binge eating accompanied by a sense of loss of control over eating without inappropriate compensatory behaviors. Because people with BED more commonly seek treatment for the psychological and medical factors that are associated with the disorder, patients’ first point of contact with the medical profession is likely to be the primary care physician (PCP). The PCP’s role includes making efforts to screen for BED symptoms, employing motivational interviewing strategies to enhance likelihood of following through with treatment, providing psychoeducational information about eating and weight control, monitoring eating, weight, and related medical problems at follow-up visits, and making referrals to behavioral health specialists who can deliver empirically supported treatments for BED.
- Conclusion: Proper screening and referral in the primary care setting can optimize the likelihood that patients obtain empirically supported treatment.
BED is the most common eating disorder, but it is one for which many do not seek treatment directly. Rather, those struggling with BED more commonly seek treatment for the psychological and medical factors that are strongly associated with the disorder. As will be reviewed below, these factors include poor social adjustment, functional impairment, psychological distress and psychiatric comorbidity, and myriad medical sequelae due to obesity and weight cycling. As such, the BED patient’s point of first contact with the medical profession is most likely to be with the primary care physician, who has several roles in the treatment of BED. There is a limited evidence base for pharmacological treatment of BED, with some medications yielding short-term reductions in binge eating, but none with strong support for long-term efficacy [4]. However, with the recent FDA approval of lisdexamfetamine dimesylate for the treatment of moderate to severe BED, this picture may change. Nonetheless, pharmacologic interventions for comorbid medical conditions will fall solidly in the bailiwick of the primary care physician. In addition, the primary care physician’s role includes making efforts to screen for BED symptoms; employing motivational interviewing strategies to enhance likelihood of following through with treatment; providing psychoeducational information about eating and weight control; monitoring eating, weight, and related medical problems at follow-up visits; and making referrals to behavioral health specialists who can deliver empirically supported treatments for BED. Finally, because BED is typically associated with weight gain over time [5], the primary care physician is encouraged to reinforce the clinical significance of weight maintenance as opposed to necessarily promoting a goal of weight loss. The rationale for this primary care approach is reviewed below, in consideration of the scientific literature and a case study highlighting common clinical features.
Case Study
Initial Presentation
A 35-year-old Caucasian woman schedules an appointment for her annual physical examination with her primary care physician. She reports generally good health but complains of low mood, joint pain, and difficulties managing her weight. Her blood pressure is managed with 100 mg/day of metoprolol. The only other medication she takes is birth control (ethinyl estradiol 20 mcg).
Physical Examination
During physical examination, it is determined that the patient is 5'6" and weighs 286 lb, with a body mass index (BMI) of 46.2 kg/m2, placing her in WHO obesity class III. The patient’s blood pressure is 130/85 mm Hg (medically managed), and her heart rate is 83 bpm. The patient states that she has been experiencing episodes of low mood off and on most of her life; she recently ended a relationship, which has exacerbated her symptoms. The physician states that the patient has gained a significant amount of weight since her last physical examination. The patient reports that she quit smoking 6 months ago and has since gained approximately 30 lb; she has considered smoking again to manage her weight.
• What are the diagnostic criteria for BED?
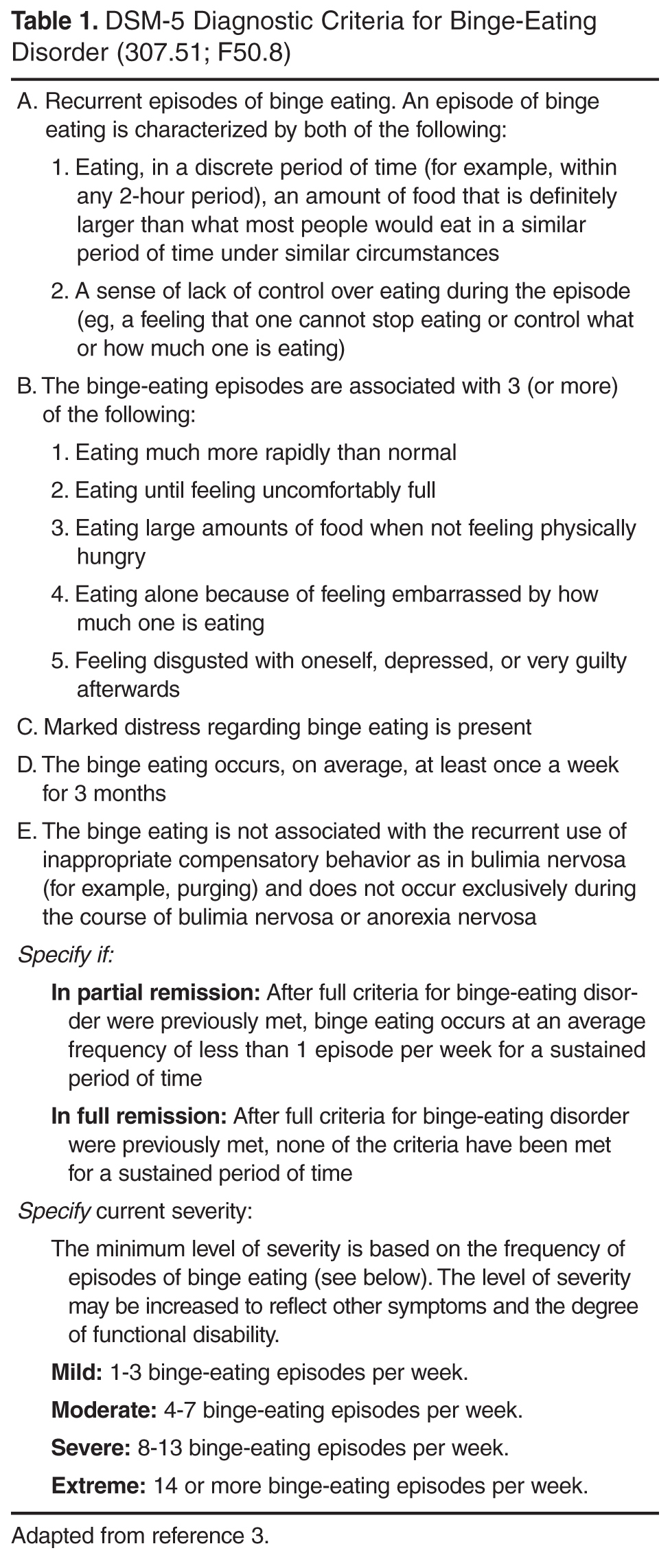
BED diagnostic criteria (Table 1) have been closely examined for their validity and clinical utility, and several have been the subject of intense debate in the BED literature. The first BED criterion, recurrent episodes of binge eating, refers to 3 essential components: amount of food, time period, and a subjective experience of loss of control. The majority of debate regarding this criterion revolves around the requirement for consumption of a “large amount of food.” There are 2 primary arguments against this criterion. First, it is inherently subjective and requires the person making the diagnosis to distinguish between normative food intake and excessive food intake [6]. There is also some debate as to whether or not individuals with BED actually consume large amounts of food when they binge. However, research supports that those with BED may consume over 1000 kcal during binge episodes, far more than those without BED who are asked to binge eat in the lab [7,8].
Nonetheless, a distinction has been made between objective binge-eating episodes (OBE) and subjective binge eating episodes (SBE) [9]. OBEs are binge eating episodes that meet the full criteria including a large amount of food and a subjective loss of control. SBEs, in contrast, are binge eating episodes that include a subjective loss of control but not a large quantity of food. If consumption of a large quantity of food is essential to the underlying pathology of BED, one would expect that OBEs and SBEs would be associated with different clinical characteristics. However, several studies have failed to find significant difference between individuals reporting OBEs and SBEs with regard to age, age of BE onset, BE severity, interpersonal problems, depressive symptoms, generalized psychopathology, and ED-related psychopathology [10–13]. Results regarding prognosis are mixed, with some suggesting that SBE more readily responds to placebo, while others suggest that SBEs are slower to remit than OBEs [11,13,14]. With respect to primary care, this literature suggests that it is not necessary for busy primary care physicians to devote time to understanding the amount of food consumed by the patient; if the patient perceives that her eating is out of control and excessive, that can generally be considered valid data in terms of considering a BED diagnosis, particularly when combined with even moderately overweight status.
In contrast to the controversy regarding amount of food, the majority of studies suggest that BED binge eating episodes fall within the 2-hour duration specified by the DSM-5 criteria, although longer durations have been reported [13]. The loss of control (LOC) criterion also appears to be relatively well-supported across studies [13,14]. LOC is a key defining feature of a binge eating episode for individuals with and without BED [15–18].Furthermore, the emotional distress associated with loss of control has been associated with depressive symptoms, appearance dissatisfaction, and poorer mental health-related quality of life [19]. In contrast, one study found that 18.6% of self-reported binges were not associated with loss of control [20]. Of note, there is some concern that the focus on LOC in the diagnostic criteria may lead to under diagnosis of BED among men, as women with BED were more likely than men to identify LOC as a core aspect of a binge eating episode [17].
The second DSM-5 criterion for BED requires that BE episodes be associated with 3 or more of the following: (a) eating more rapidly than normal; (b) eating until uncomfortably full; (c) eating large amounts of food in the absence of hunger; (d) eating alone because of embarrassment about how much one is eating; and (e) feeling disgusted with oneself, depressed, or very guilty after overeating. This criterion is not as controversial as the first, and has correspondingly not received as much attention in the BED literature. However, results from a handful of studies provide some support for their inclusion, particularly in light of the fact that individuals are only required to endorse 3 of the 5 symptoms [13–15,17,21].
The third criteria for BED requires that individuals experience “marked distress” about BE. Only one known study has directly evaluated the distress criterion, and its validity was confirmed by results that suggested individuals with full-threshold BED had significantly greater ED-related psychopathology and depressive symptoms as compared to individuals who met all but the distress criteria for a BED diagnosis [22].
The fourth criteria for BED stipulates that BE occurs an average of once a week for 3 months. Previously, DSM-IV-TR required more frequent episodes, at least 2 days a week for 6 months, but this was criticized as lacking in empirical basis [23]. The current state of the evidence suggests that, with regard to frequency of BE episodes, BED best fits a continuous model rather than a categorical model. That is, symptoms and related impairment exist across a severity spectrum as a function of how often BE episodes occur. For example, in a critical review, Wilson and Sysko noted that individuals with sub-threshold frequency of BE episodes had less severe psychopathology than those meeting criteria for DSM-IV BE frequency (ie, at least 2 days a week for 6 months), but they were still significantly more impaired than those who did not binge eat [24]. The authors asserted that there was no empirical rationale for preserving the criteria of 2 binge days per week for 6 months, and indeed, DSM-5 adopted a more relaxed standard. As is the case with symptoms of many psychological disorders, there does not appear to be a definitive and concrete point at which binge eating becomes pathological [23]. Fortunately, reliability for the new criteria is good and appears superior to the DSM-IV criteria [25].
Finally, the last criteria for BED—which remains unchanged from the provisional criteria in DSM-IV-TR —is essentially a rule-out that states that BE should not be accompanied by the regular use of “inappropriate compensatory behaviors” or exclusively occur during the course of anorexia or bulimia. These criteria have also been criticized as being subjective, particularly in light of the fact that individuals with BED often report a history of infrequent purging behavior and frequently engage in weight-loss attempts [6,13,14]. However, the need for a rule-out is clear given that BE also occurs during the course of bulimia and anorexia, binge-eating/purging type, and it is supported by the low rates of crossover from BED to bulimia and/or anorexia [26].
Remission and severity specifiers are new to DSM-5. With respect to the latter, a recent study observed small but significant elevations in eating pathology among those with moderate severity BED, relative to the eating pathology experienced by those with mild severity, but there were no differences in level of associated depression. Interestingly, a better differentiator of severity of eating pathology and depression among patients with BED was overvaluation of shape/weight [27]. As such, the primary care physician might be better advised to focus on indicators of this important variable by querying the extent to which the patient’s shape and weight have influenced how she feels about (judges/thinks/evaluates) herself as a person, rather than using the number of BED symptoms alone as the indicator of severity.
• What is the epidemiology of BED?
Based on DSM-IV-TR criteria, the overall lifetime prevalence rate for BED has been reported to be 2.8%, and it is more common in women (3.5%) than men (2%) [28]; the overall 12-month prevalence rate is 1.2% (1.6% in women and 0.8% in men) [28]. Using DSM-5 criteria, a recent study observed that lifetime prevalence of BED by age 20 was 3.0% for BED and an additional 3.6% for subthreshold BED, with peak age of onset (for both) between ages 18 to 20 years [29]. Notably, even though prevalence rates are slightly higher using DSM-5 criteria (presumably, due to the relaxed criteria for frequency and duration of binge eating), effect sizes for impairment are also higher, suggesting that the revised criteria are not identifying BED cases marked by less impairment [29]. Although often thought of as a disorder common among young women, BED prevalence among middle-aged women (40–60 years) has a prevalence of at least 1.5%, with additional subthreshold cases being common in this age-range; groups meeting full BED criteria and subthreshold cases are both characterized by high levels of distress and impairment [30].
Gender Differences
Men engage in overeating as much or more than women but are less likely to endorse a loss of control and/or distress associated with BE [28,31], and thus are less likely to meet full BED criteria. However, when men do meet criteria for BED, they experience as much clinical impairment as their female counterparts [32]. Additionally, men’s BE may be more directly affected by body image dissatisfaction than women’s BE, and although it is associated with negative affect, it is less likely to be associated with interactions between negative affect and dietary restraint than seems to be the case for women [33]. In addition, in the primary care setting, men with BED were strikingly similar to their female counterparts on most historical and developmental variables [33]. However, men reported more frequent strenuous exercise, whereas women reported that onset of overweight and dieting occurred earlier in life [34]. That same study observed that men (57%) were more likely than women with BED (31%) to meet criteria for metabolic syndrome, even after controlling for race and BMI. A second study by the same research group again demonstrated that men with BED are more likely to show elevated blood pressure, triglycerides, and meet criteria for metabolic syndrome, whereas women are more likely to have elevated total cholesterol [35].
Race/Ethnicity
The evidence related to rates of BED among ethnic minorities is equivocal, with some studies demonstrating that Caucasian women are more likely to experience clinical levels of BED symptoms [36,37], others finding comparable rates between Caucasian and African-American women [38,39], and still others discussing the possibility of finding the greatest rates of binge eating in ethnic minority samples [40], especially in light of the high rates of obesity observed in some ethnic minority groups [41,42]. Studies that focus on subclinical levels of eating pathology among undergraduate students are most likely to find significant ethnic differences, while studies of nonclinical samples utilizing diagnostic threshold find the fewest differences [43]. There is at least some research demonstrating the highest rates of body image disturbance or eating problems among Asian Americans [44,45]. In addition, Latino individuals with BED may have higher levels of ED-related psychopathology as compared with Caucasian individuals [46]. Finally, Caucasian individuals who experience BED may be more likely to utilize mental health services as compared with other ethnic groups [47].
Age
Lower rates of BED have been documented in elderly individuals relative to their younger counterparts in population-based studies [28]. However, this may be due to recall bias, birth cohort effects, restricted access to studies, and/or increased medical morbidity leading to premature mortality [48]. Guerdjikova et al [48] also noted that many treatment outcomes studies have exclusion criteria related to age. This is unfortunate, as elderly individuals and their younger counterparts appear to exhibit similar levels of BE behavior, distress due to BE, weight and shape concerns, psychiatric comorbidity, and obesity. However, elderly individuals have reported later onset, longer duration of illness, and less medical morbidity [48]. In another study, Mangweth-Matzek et al [30] surveyed women between the ages of 40 and 60; they found that very few respondents met full criteria for an eating disorder. However, when criteria were relaxed (ie, dropping associated symptomology for BED and frequency criteria for bulimia nervosa) an additional 4.8% of the sample met criteria. Notably, women with subthreshold eating disorders reported very similar levels of comorbid psychopathology as women whose symptoms met diagnostic criteria.
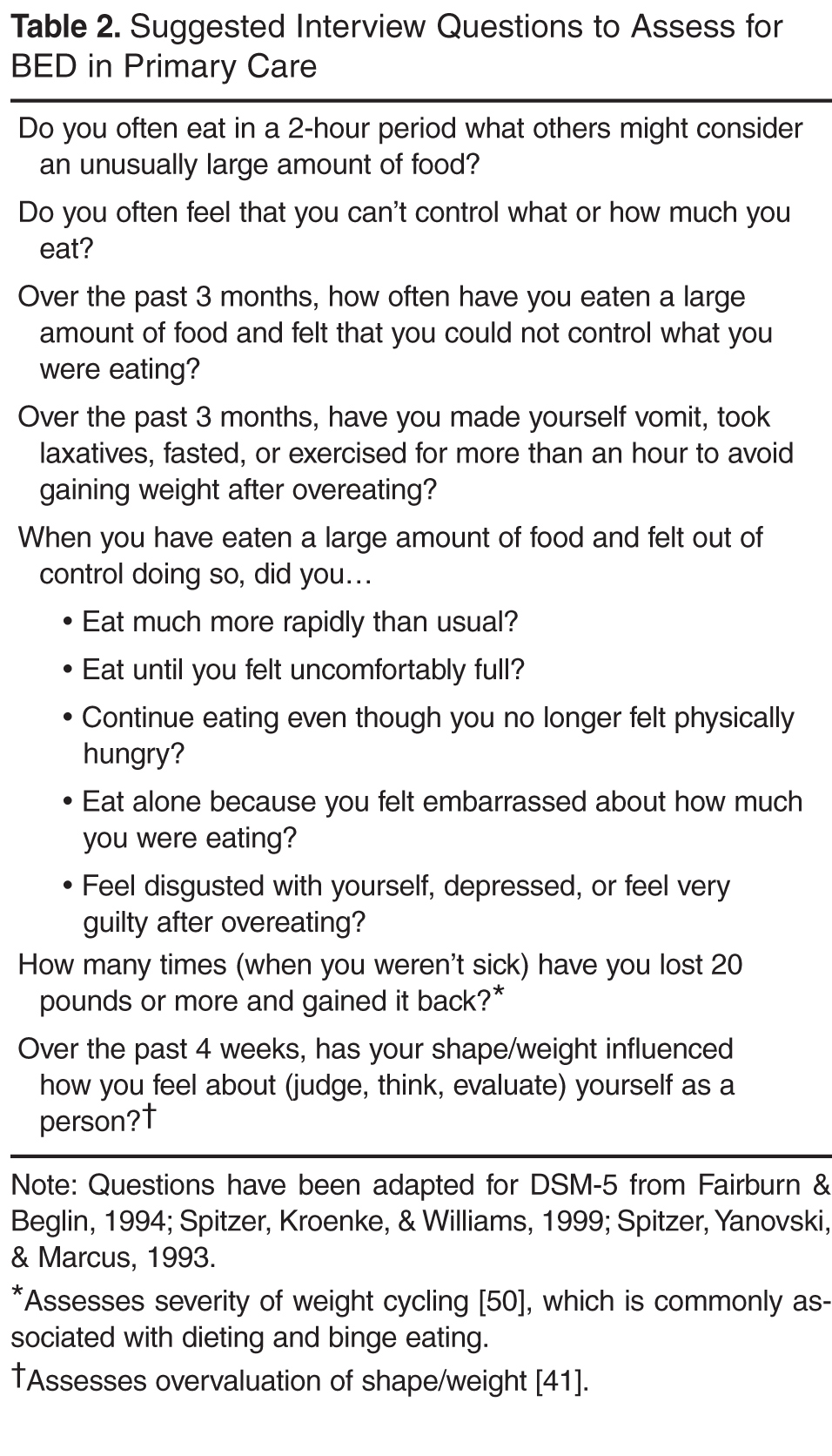
• What tools are available for assessment of BED in the primary care setting?
Two of the most commonly used questionnaires in specialty clinics are the Eating Disorders Examination– Questionnaire (EDE-Q [49]), and the Questionnaire on Eating and Weight Patterns – Revised (QEWP-R [50]). In the primary care setting, both appear to be low-cost and time-efficient methods of screening for BED. The EDE-Q, however, may underestimate frequency of binge eating episodes and overestimate the extent of eating-related pathology [51]. Notably, the QEWP has been revised to reflect DSM-5 criteria and is available free of charge (QEWP-5 [52]). The Binge Eating Scale [53] is a 16-item scale often used to assess severity of binge eating; it is free and easily accessible online. Regardless of what measure is used, research indicates that a higher proportion of people agree to having episodes where they ‘‘lose control over eating’’ than when asked about having episodes of ‘‘binge eating’’ [54], so asking about loss of control over eating might be the more advisable way to open the discussion with patients about their eating behavior. In assessing for binge eating, physicians should also be aware of some of the differences in clinical presentation observed for ethnic minorities (eg, lower drive for thinness among African-American women) as well as some research demonstrating that measures such as the Eating Disorder Diagnostic Scale do not assess equivalent constructs in African-American and Caucasian clients [55]. Finally, while self-report measures often serve a practical function of quickly assessing a large group, physicians may want to consider relying on interview-based techniques for clients with lower levels of education attainment and literacy; at least one study has demonstrated problems with readability and comprehensibility with most BED measures [56].
• What are the clinical features of BED?
BED and Obesity
The specific impact of BED on health is difficult to separate from the impact of obesity on health, as the two conditions frequently co-occur and are confounded in many studies. Of relevance to the primary care setting, many BED patients report gaining a substantial amount of weight in the year prior to seeking treatment [57].
Although individuals with BED are often obese, proponents of classifying BED as a separate DSM diagnosis argue that individuals with BED differ from their non-BED obese counterparts in regards to eating patterns, eating disordered psychopathology, and associated features and comorbidities. Individuals with BED consume more calories in laboratory studies than weight-matched controls [6,7,58]. In contrast, studies utilizing ecological momentary assessment (ie, real-time assessments) found no differences between BED obese and non-BED obese participants in the frequency of self-reported binge eating and caloric intake during binge eating episodes [59,60]. BED participants, however, were more likely to report higher stress, desire to binge, negative affect, dietary restraint, and being alone immediately before self-reported binge eating episodes. Furthermore, individuals with BED also demonstrate more ED-related psychopathology than non-BED obese individuals [61–63]. Psychiatric comorbidity is also higher among BED obese individuals as compared their non-BED obese counterparts, and the increased comorbidity is accounted for by the severity of binge eating as opposed to the severity of obesity [6,64–67]. In addition, research demonstrates that obese individuals with BED, as compared with non-obese BED patients, have a poorer quality of life [68].
BED and Bulimia Nervosa
Numerous studies have supported the distinction between bulimia nervosa and BED [69–76]. Diagnostically, bulimia nervosa differs from BED by its requirement of recurrent inappropriate compensatory behaviors in order to prevent weight gain, such as self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise [3]. BED and bulimia nervosa are distinguished by distinct risk factors, prevalence, course, and treatment outcomes [28,67,77]. Individuals with BED are less likely than individuals with bulimia to diet before onset of the disorder, and fewer individuals with BED cross over into other ED diagnostic categories [26,78–81]. Finally, BED and bulimia nervosa are associated with different constellations of ED-related symptoms and associated features [28,63,79]. For example, relative to BE patients, those with bulimia show greater work impairment and psychiatric comorbidity [28], higher dietary restraint and eating concerns [63], and lower rates of obesity [79].
Psychiatric Comorbidity
BED is associated with poor social adjustment, greater functional impairment, and significant psychiatric comorbidity, including overall distress and suicidality [67]. In a study of comorbidity with only selected disorders (mood, anxiety, impulse-control, and substance use disorder), 78.9% of individuals with BED had a lifetime history of at least one comorbidity, 20.2% had one comorbid disorder, 9.8% had two, and 48.9% had three or more [28]. Furthermore, the presence of current psychiatric comorbidity is associated with greater ED-related psychopathology and associated distress [40,41]. The most common comorbidities (lifetime rates) are specific phobia (37.1%), social phobia (31.9%), major depressive disorder (32.3%), post-traumatic stress disorder (PTSD) (26.3%), alcohol abuse/dependence (21.4%), conduct disorder (20%), attention-deficit/ hyperactivity disorder (19.8%), illicit drug use/dependence (19.4%), and oppositional-defiant disorder (18%) [28]. A recent report supports that this level of comorbidity is evident in primary care settings, noting that PTSD in particular is common and associated with a host of other difficulties, including depression, anxiety, drug use disorders, greater eating disorder pathology, and poorer psychological functioning [82]. Personality disorders are also commonly comorbid with BED, with the highest lifetime rates for avoidant (11%), obsessive compulsive (10%), and borderline (9%) personality disorders [83]. Finally, cigarette smoking is also associated with binge eating [83,84], likely evolving out of a weight-control smoking profile [85], and this is of relevance to the primary care setting in that smokers with BED gain more weight upon smoking cessation than do their non-BED counterparts [86].
Further Evaluation
To assess behavioral factors related to obesity and recent weight gain, the physician asks the patient if she ever eats what would be considered an unusually large amount of food for the circumstance. The patient acknowledges that she does so regularly, particularly in response to negative moods. The patient also describes that these episodes contribute to ongoing low mood, such that she feels highly depressed and hopeless following binge episodes. The physician then asks about the patient’s exercise habits and weight management techniques. While the patient denies engaging in compensatory behaviors (eg, vomiting, laxative use) to counteract excessive eating, she does report a history of dieting in which she dramatically restricts her food intake and subsequently loses weight. The patient states that these periods are inevitably followed by a resumption of overeating, and she typically gains back more weight than she originally lost. The patient estimates that she has lost and regained more than 20 lb at least 5 times during her lifetime. In addition, the patient reports difficulty maintaining a regular exercise regimen, especially since the onset of osteoarthritis-related joint pain in the past year. After the evaluation, the physician orders an electrocardiogram (ECG) and blood work. The ECG shows that the P-wave, QRS, and T-wave axes are shifted leftward, but within normal limits. A follow-up appointment is scheduled in 2 weeks.
• What are the medical complications of BED?
BED is associated with numerous negative health sequelae including obesity, sleeping problems, musculoskeletal pain, joint pain, headaches, gastrointestinal problems, menstrual problems, shortness of breath, chest pain, diabetes, low health-related quality of life, and functional health impairments [87–90], with many of these risks persisting even after controlling for BMI [91]. A 5-year follow-up of 134 individuals with BED and 134 individuals with no history of eating disorders, who were frequency-matched for age, sex, and baseline body mass index (BMI), provides further support that BED confers risk of components of metabolic syndrome beyond the risks associated with BMI alone [92]. Specifically, BED cases had higher longitudinal risk of developing dyslipidemia, hypertension, type 2 diabetes, any metabolic syndrome component, and two or more metabolic syndrome components. Alarmingly, these findings even emerge in studies of pediatric samples, wherein BED predicts development of metabolic syndrome, elevated triglycerides, and increases in visceral adiposity [93].
• What are risk factors for BED?
A number of risk factors for BED have been identified, although many are risk factors for a number of psychiatric disorders and not specific to BED. These general risk factors include depression/negative affectivity [94,95], parental mood and substance use disorder, maternal problematic parenting, and separation from parents [95]. A host of risk factors have been identified for disordered eating, in general, including body dissatisfaction [94], early onset of dieting [94], and perfectionism [96]. A number of other variables are risk factors for both BED and bulimia (but not anorexia), including a history of childhood bully and teasing, negative self-evaluation, parental depression, and negative family communication about shape and weight [81,96]. In a study comparing BED cases to psychiatric controls, childhood obesity, familial eating problems, family discord, and high parental demands differentiated the BED cases [95]. In summary, it has been suggested that BED risk is conferred by factors that increase risk of psychiatric disorder in general and those that confer risk for obesity [81]. Of note, the risk factors studied do not appear to differ between black and white women [95].
Genetic risk factors appear to play a strong role in the development of BED. Risk for BED tends to aggregate in families independently of the risk for obesity, although the presence of BED in a first-degree relative does increase risk for obesity [97]. Heritability estimates for BED range from 45% to 57% [98,99], which is greater than the heritability estimate for subthreshold binge eating (ie, overeating with a sense of loss of control, 41%) [100]. In addition, symptom-level analyses support moderate genetic contributions for each BED symptom [98], supporting the integrity of the diagnostic criteria. Finally, shared environment appears to play a very small role in the familial transmission of BED, and the contribution of unique environmental factors in development of BED appears to be substantial [97,101].
With regard to the neurobiological underpinnings of BED, it appears that BED may be associated with hypersensitivity to reward, a phenomenon that is strongly associated with the striatum and dopaminergic mechanisms [102,103]. In support of this hypothesis, Davis et al [102] reported that BED was differentially related to genotypes that reflect a greater density of D2 receptors and higher D2 binding potential as compared to obese controls. Additionally, greater increases in striatal DA and unique activation patterns in the right ventral striatum have been demonstrated in individuals with BED as compared to obese non-BED controls in response to food-related stimuli [103,104]. Other findings have implicated the orbitofrontal cortex (OFC) in BED, which is another brain region responsible for reward processing, particularly as it relates to the hedonic value of food stimuli [103]. Increased volume of grey matter has been documented in individuals with BED and bulimia as compared to normal weight controls, and stronger medial OFC activation while viewing pictures of food was observed in individuals with BED as compared to individuals with bulimia, overweight controls, and normal controls [105].
Difficulties with affect regulation have also been implicated in the development of BED. Two theories that implicate a primary and specific role for affect regulation in BED are cited most frequently in the extant literature: the affect regulation theory and the escape theory. The affect regulation theory [106] posits that BE is a conditioned response to negative affect which is correspondingly negatively reinforced by reductions in negative affect, which could occur during or after BE. Escape theory [107] posits that aversive self-awareness causes negative affect, which in turn triggers BE. BE is then negatively reinforced by reductions in negative affect during a binge via an escape from self-awareness that is accomplished through cognitive narrowing to the immediate stimulus environment. In contrast to the affect regulation theory, escape theory predicts that negative affect will increase after BE when self-awareness is restored. Results regarding changes in affect during BE episodes are conflicting as to whether BE is associated with decreases, no change [108–110], or even increases in negative affect. In particular, a meta-analytic review of 36 studies that examined affect via ecological momentary sampling found moderate increases in negative affect following binge episodes [111]. To some degree, results of this meta-analysis may not generalize to BED, per se, given that it included other binge eating groups, such as those with bulimia nervosa. However, in general, studies suggest that negative affect is an antecedent for BE and increased negative affect may be a consequence of BE, at least among women. More information is needed regarding aversive self-awareness before and after BE, cognitive narrowing, and changes in affect during BE. As such, the current state of the literature provides only partial support for affect regulation models of BED in women. Furthermore, it remains unknown if these results will generalize to men.
Clinical Course
Evidence regarding the course and stability of BED is conflicting and unclear. Several prospective studies have suggested that BED is not a stable disorder, exhibiting high rates of remission over time [26,99,112]. However, the samples have been criticized for being small, completely female, younger than typical individuals with BED, and post-ED treatment. In contrast, a prospective study that included older women and a combination of treated and untreated women suggested remission rates at 1 year that were much lower (7%) [78]. Additionally, a retrospective study [113] reported an average BED duration of 14.4 years. In a review of the studies cited above, Wonderlich et al [6] concluded that “[a]lthough there is variability in the data, it does appear that BED differs from other eating disorders in terms of a greater tendency toward recovery and fluctuation, although this may be embedded in a chronic pattern of remission and relapse.” Viewing BED as a disorder with a chronic pattern of remission and relapse could explain why individuals with BED retrospectively report a longer duration of illness, as they may be more likely to conceptualize their illness as one continuous course punctuated by different periods of severity rather than several distinct bouts of BED. Finally, although diagnostic crossover is a frequent phenomenon among other eating disorders, the crossover rate for BED appears relatively low as compared to anorexia and bulimia [6,26,28,66].
Follow-up
Laboratory examination shows TSH levels within normal limits and cholesterol levels of 48 mg/dL(HDL), 162 mg/dL (LDL), and 270 mg/dL (total). Triglyceride levels are 300 mg/dL and the patient’s fasting glucose level is 115 mg/dL. At the patient’s follow-up appointment, the physician states that a number of laboratory results indicated negative weight-related health consequences, including high cholesterol, high triglycerides, hypertension, and probable pre-diabetes. The patient initially disregards the significance of these results, stating she only gained weight due to her break-up and quitting smoking, and she is motivated to diet to lose weight in the near future. The physician asks for more information about the patient’s eating behavior, in particular asking if she ever feels as if she loses control over her eating. The patient reluctantly admits to this, and the physician provides a referral to a behavioral health specialist. The patient expresses ambivalence and a desire to try to manage her weight on her own. The physician uses motivational interviewing techniques to enhance motivation to follow up on this referral. In addition, the patient is encouraged to make small changes to her diet and slowly increase her exercise by taking walks. Another follow-up appointment is scheduled in 3 months.
• Which treatments are most effective for BED?
Despite the negative sequalae of BED, studies suggest that it often goes untreated [114]. Women with BED, as compared to women with anorexia and bulimia, are less likely to seek treatment for BED and less likely to receive treatment for their eating disorder when they do seek it out [114–116]. Barriers to treatment may include shame and internalized weight stigma, lack of knowledge about where to seek treatment, a belief that willpower should be sufficient to overcome the problem, lack of understanding that BED is a psychiatric disorder, finances/insurance barriers, and lack of BED detection by non-specialist treatment providers [115]. These barriers are particularly concerning, as women with BED report greater health care utilization and comprise a large segment of patients in weight control programs. Therefore, it appears individuals with BED seek help for the negative consequences of the disorder, but they are less likely to seek and receive help for the likely root cause of their concerns. This is a particularly damaging pattern, as the presence of BED may negatively impact the outcome of obesity treatment [117]. There are, however, a number of promising treatments for BED, as described below:
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is generally considered to be the most well-established and empirically supported treatment for BED [118,119]. The cognitive behavioral conceptualization of BED is based on Fairburn, Cooper, and Shafran’s [120] transdiagnostic model of eating disorders (CBT-E), which is an expanded version of the cognitive behavioral model of bulimia nervosa [121]. CBT-E posits that the core pathology in eating disorders is a dysfunctional system in which self-worth is based on eating habits, shape, or weight, and the individual’s ability to control them. Attempts to maintain self-worth by controlling eating, shape, and weight result in extreme and brittle forms of dietary restraint. Inevitable violations of the individual’s dietary rules are then interpreted as lack of self-control, leading to a temporary abandonment of dietary restraint and consequent BE. These dietary slips and corresponding BE often occur in response to acute changes in mood, and BE is thus negatively reinforced by “neutralizing” negative mood states. Lapses in dietary restraint also result in secondary negative self-evaluation, which serves to further exacerbate a cycle of increased dietary restraint to improve self-worth and then inevitable dietary lapses leading to BE. CBT-E expanded upon CBT-BN by postulating 4 processes that maintain ED: severe perfectionism (clinical perfectionism), unconditional and pervasive low self-esteem (core low self-esteem), difficulties coping with intense mood states (mood intolerance), and developmental interpersonal difficulties (interpersonal difficulties). Of note, the CBT-E model explicitly states that individuals may differ in the extent to which they experience the 4 maintaining processes and not every individual will experience all four.
Overall, treatment is focused on normalizing eating patterns (ie, not weight loss), cognitive restructuring for weight/shape concerns and other triggers for binge eating, and relapse prevention [122]. CBT has produced substantial reductions in binge eating as compared to no treatment [123–125] and supportive therapy [126]. The majority of RCTs have reported remission rates greater than 50% [127]. Unfortunately, CBT has generally not produced meaningful weight loss [118,122,127–129], but this may be a contraindicated goal. CBT has demonstrated improvements in a number of features associated with BED including eating disordered psychopathology [122,124,130,131], depression [122,124,130,132], social adjustment [133], and self-esteem [132]. Treatment gains are generally well-maintained at 1-year to 4-year follow-up [122,123,130,133,134]. Individual and group treatments appear to produce similar results [134], and treatment completion rates have been estimated at approximately 80% across different delivery formats [127]. One strength of the CBT literature is the inclusion of participants with severe psychopathology, which facilitates the generalizability of these findings [127].
A number of factors have been associated with treatment outcome in CBT trials. Poor treatment outcomes have been associated with a history of weight problems during childhood, high levels of emotional eating at baseline, interpersonal dysfunction, and low group cohesion during group CBT [110,124,134]. Overvaluation of weight and shape demonstrated a statistical trend toward negatively impacting outcomes in one study. The presence of a cluster B personality disorder (ie, borderline histrionic, antisocial, and narcissistic personality disorders) predicted higher levels of binge eating at 1-year follow-up in a combined sample of participants treated with group CBT or group interpersonal psychotherapy (IPT) [135].
Alternatively, positive treatment outcomes have been associated with low levels of emotional eating at baseline, older age of onset, weight loss history that is negative for amphetamine use, and decreases in depressive symptoms during treatment [124,134,136,137]. In addition, early response to treatment (defined as a 65%–70% reduction in binge eating within 4 weeks of starting treatment) tends to be associated with greater long-term (ie, 1–2 year) remission from BED and lower eating disorder psychopathology, across a variety of psychological treatment approaches [138–144].
Interpersonal Psychotherapy
IPT for BED was adapted by Wilfley and colleagues [145] from IPT for depression, and the rationale for its use with BED is based on successful outcomes for individuals with bulimia and multiple studies documenting interpersonal deficits in individuals with BED [146]. IPT seeks to address interpersonal problems in 4 areas: interpersonal conflict, grief, role transitions, and interpersonal deficits [135]. While adapting IPT for BED, it was noted that the course of BED tends to be more chronic than the course of depression, thus the focus of IPT for BED was shifted from addressing the interpersonal precipitants of the disorder to the interpersonal factors that maintain the disorder [145]. Fewer studies examining the effectiveness of IPT in treating BED have been published than those examining CBT for BED, but it appears that IPT is as efficacious as CBT immediately post-treatment [130], and at 1- [130] and 4-year follow-up [147]. In addition, at least 2 studies have been published that compare IPT, cognitive behavioral therapy–guided self-help (CBTgsh), and behavioral weight loss [133,141]. Overall, results support the use of both IPT and CBTgsh (discussed in more detail below), with important moderators of treatment effects observed. For example, Wilson et al [133] found that clients with higher levels of psychopathology were better suited for IPT. The authors conclude that these results could inform a model of evidence-based stepped care, where CBTgsh, a low-cost, low-intensity treatment, should be considered as the first line of treatment. Secondarily, IPT, which represents a more specialized and expensive form of treatment, could be considered the next level of care, particularly for clients who are not demonstrating rapid improvement in response to CBTgsh.
Dialectic Behavior Therapy
A small number of studies have investigated the treatment of BED with dialectical behavior therapy (DBT). Originally developed to treat borderline personality disorder [148], DBT is of particular interest given its explicit targeting of emotion regulation. According to the DBT model of BED [149], emotional dysregulation is the core psychopathology in this disorder, and binge eating is viewed as attempts to influence, change, or control painful emotions. Initially, promising results were published showing positive treatment effects in an uncontrolled study [150] as well as wait-list controlled trials [151]. Notably, relative to wait-list controls, participants in a DBT guided self-help program (who received an orientation, DBT manual, and six 20-minute support calls across 13 weeks) reported reduced past-month binge eating, higher binge eating abstinence rates, and over the longer term improved quality of life and reductions in ED psychopathology. However, a comparison of DBT-BED with an active comparison control group (ie, nonspecific supportive therapy) failed to find significant differences between the 2 treatments (defined as effect size greater than 0.5) at 12-month follow-up in binge eating abstinence, binge eating frequency, most ED-related psychopathology, positive affect, depression, and self-esteem [152]. Therefore, DBT may have potential and, at a minimum, is equally efficacious as supportive therapy.
Mindfulness- and Meditation-Based Therapies
Treatment outcome studies utilizing mindfulness-based therapies, including mindfulness-based stress reduction (MBSR) and acceptance and commitment therapy (ACT), make up a small but promising body of literature. Reasoning that negative affect, eating in the absence of hunger, and emotional eating may comprise one pathway to binge eating [153,154], it follows that mindfulness-based therapies may act through their effects on emotion regulation, acceptance strategies for tolerating negative affect, and awareness of bodily cues. A recent review identified 19 studies exploring the effects of mindfulness-based interventions on binge eating severity and frequency as well as a number of related indicators, observing positive effects for this form of treatment [155]. For example, MB-EAT [156] is a group treatment for BED that is primarily based on MBSR. Treatment is targeted at cultivating mindfulness, mindful eating, emotional balance, and self-acceptance[157]. The treatment also places particular emphasis on developing self-awareness of internal hunger and satiety cues. A recent randomized controlled trial of MB-EAT produced significant improvements in binge eating frequency and BE-related psychopathology [158]. Furthermore, process variables including hunger awareness, satiety awareness, and mindfulness were correlated with positive outcomes. In addition, a small study (n = 39) that compared ACT to standard follow-up utilized by a bariatric surgery team demonstrated significantly greater improvements in disordered eating, body satisfaction, and quality of life for clients who participated in ACT [159]. In brief, results suggest that mindfulness-based interventions represent an additional treatment approach with supporting but limited evidence to date.
Self-Help Interventions
Self-help interventions for BED are categorized as pure self-help or guided self-help. In treatment outcome studies, pure self-help is generally conducted with a self-help manual, although several studies have examined more novel formats such as the internet, video, and CD-ROM. GSH also uses a self-help manual (or other format) with the addition of brief sessions with health care providers who have varying degrees of expertise with the type of therapy being utilized. CBT is the most commonly utilized therapeutic modality in treatment outcome studies of self-help interventions, and they most often utilize Fairburn’s Overcoming Binge Eating self-help manual [160].
Two studies have directly compared pure and guided self-help with Fairburn’s manual and produced conflicting results. Carter and Fairburn [161] found that in a sample of primarily white women with BED, pure self-help (CBTsh; n = 24) and guided self-help (CBTgsh; n = 24) were equally effective, and both were superior to wait-list controls at 6-month follow-up in producing BE abstinence (CBTsh = 40%, CBTgsh = 50%), reducing binge eating, ED-related psychopathology, and general psychiatric symptoms. In contrast, a study comparing CBTsh and CBTgsh in 40 primarily white women with recurrent binge eating (82.5% diagnosed with BED), guided self-help was superior to pure self-help at the end of treatment in reducing BE frequency, eating concern, and restraint [162]. CBTgsh and CBTsh were equally effective in producing BE abstinence (50% and 30%, respectively), and reducing shape concern, weight concern, and general psychiatric symptoms [162]. Higher levels of general psychiatric symptoms were predictive of higher BE frequency post-treatment for both treatments. It should be noted that participants in both conditions experienced statistically significant improvements on all variables as compared to baseline.
CBTgsh also performed as well or better than individualized treatments in one study [133]. CBTgsh, IPT, and behavioral weight loss (BWL) were compared in a large study of 205 primarily white, obese or overweight individuals diagnosed with BED. The 3 treatments produced equivalent outcomes for binge eating at post-treatment, but BWL produced significantly greater weight loss. However, at 2-year follow-up, the CBTgsh and IPT groups had maintained treatment gains and were significantly superior to BWL in reductions in binge eating. The 3 groups were equivalent with regard to weight loss at the 2-year follow-up, and none reported clinically significant weight loss. Of note, as compared to the IPT and BWL groups, the CBTgsh group received 10 sessions as opposed to 20, received 25-minute sessions as opposed to 60-minute sessions, and were treated by providers with limited levels of experience as opposed to doctoral-level clinical psychologists.
To summarize, CBT is the most often studied type of self-help treatment. Both CBTsh and CBTgsh produced improvements in binge eating and associated psychopathology as compared to baseline and wait-list controls, and treatment gains were maintained at 6-month follow-up. Conclusions regarding the relative superiority of pure self-help or guided self-help are premature given the small number of studies and conflicting results.
In addition, limited information is available regarding moderators and predictors of guided self-help outcomes. Masheb and Grilo [163] performed a cluster analysis of the sample for the CBTgsh vs. BWLgsh described above [164] and identified 2 clinically significant subtypes: a dietary-negative affect subtype characterized by high restraint, low self-esteem, and depressive symptoms; and an overvaluation of weight and shape subtype. For both the CBTgsh and BWLgsh groups, the dietary-negative affect subtype experienced higher levels of binge eating frequency, and the overvaluation of weight and shape subtype experienced higher levels of ED-related psychopathology. Additionally, individuals receiving BWLgsh who experienced a rapid response to treatment reported lower BE frequency, greater weight loss, and higher restraint than participants without a rapid response [142]. In contrast, rapid response did not appear to affect outcomes for CBTgsh participants. Finally, the combination of low self-esteem and high ED-related psychopathology negatively affected BE remission rates for CBTgsh recipients [133].
Pharmacologic Treatment
Currently only one medication, lisdexamfetamine dimesylate, has been FDA-approved for the treatment of BED. Previously approved for treating both adults and children with attention-deficit hyperactivity disorder, lisdexamfetamine dimesylate is a central nervous system stimulant and has been found to significantly reduce number of binge days, with robust effect sizes [165]. Beyond this medication, the evidence for pharmacologic treatment of BED is limited. A recent review identified only 22 studies exploring the effects of pharmacologic treatment in a methodologically rigorous way (eg, double-blind placebo design) [4]. To date, a number of different medication classes have been evaluated, including antidepressants, anticonvulsants, stimulants, anti-obesity drugs, and others. Overall, there is some evidence that antidepressant and anticonvulsant agents are efficacious at reducing BE frequency [166,167] and sometimes effective regarding statistically significant weight loss [168,169]. However, the majority of results are generally disappointing, both with respect to reductions in binge eating and sustained weight loss [48,170,171]. In addition, there are serious limitations in the literature that must be considered, including the limited number of studies that address the high placebo response observed in clinical samples, limited follow-up windows, and inadequate multiplicitious confirmatory trials. Despite these limitations, the evidence base related to pharmacologic treatment is continuously evolving and represents an important future direction for the treatment of BED.
Treatment
Prior to her next medical follow-up, the patient meets with a psychologist. The patient discloses that she has been binge eating several times per week for over a year; she also discloses a history of prolonged sexual abuse perpetrated by a step-parent during her childhood. When the patient returns to her follow-up medical appointment, she reports that her psychologist has diagnosed her with BED and PTSD. She states that they are using cognitive behavioral techniques to regulate her mood and eating behavior, with a specific aim of avoiding excessive dietary restraint. In addition, they are working together to discuss her unfulfilling romantic history and processing her experiences of trauma. Since her last appointment with the primary care physician, she reports an increased awareness of her eating habits, improvement in mood, and a 10-lb decrease in her weight.
The patient reports that she has continued to meet weekly with her psychologist and has slowly begun reintroducing low-impact exercise to her routine. She continues to lose weight gradually, but with a priority of stabilizing eating behavior and avoiding binge episodes versus aiming for weight loss. She reports that her mood has stabilized. Her cholesterol and triglycerides remain high, but her blood pressure is controlled effectively with medication. Her physician recommends continued psychological treatment, periodic meetings with a nutritionist, and prescribes medication for her cholesterol. A follow-up appointment with her physician is scheduled in 6 months.
Summary
Corresponding author: Karen K. Saules, PhD, Eastern Michigan University, Psychology Clinic, 611 W. Cross St., Ypsilanti, MI 48197, ksaules@emich.edu
Financial disclosures: None.