Improving outcomes and lowering costs by applying advanced models of in-home care





ABSTRACTWith advances in monitoring and telemedicine, the complexity of care administered in the home to properly selected patients can approach that delivered in the hospital. The challenges include making sure that qualified personnel regularly visit the patient at home, both individually and in teams; information is accurately communicated among the caregiver teams across venues and over time; and patients understand the information communicated to them by providers. Despite these challenges, the benefits of treating chronically or terminally ill patients at home are significant. Among the most important are improved patient satisfaction and reduced cost. Numerous studies have shown that most patients prefer to spend their convalescence or their last days at home. The financial benefits of enabling patients to recover or to die at home are significant.
When it can be done safely, most people prefer to be treated and recover from illness at home.1,2 Home-based services have improved considerably since Brickner called the homebound aged “a medically unreached group.”3 Still, home care has not achieved its full potential and scientific investigation of home care models is scant compared with that of other therapeutic approaches.
The challenges of studying home care include variability in interventions, difficulty defining treatment and comparison groups, and high research costs. The care itself can be demanding, requiring providers to mobilize processes that have become institution-based and immobile, integrate care across insular settings, incorporate complex social issues into the care plan, and develop a viable home care financing model.
This article reviews evidence favoring investment in advanced home care and adds perspective from 3 decades’ experience at Virginia Commonwealth University (VCU), Richmond, Virginia.
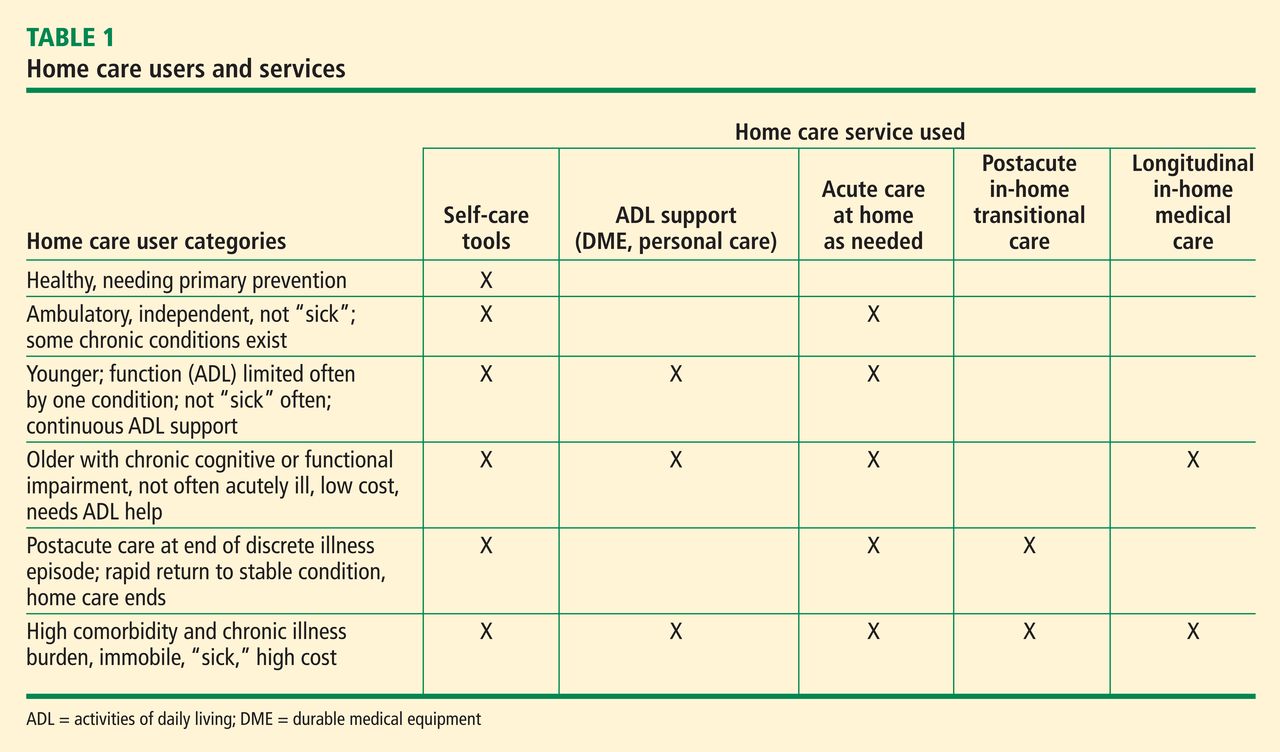
The term home care has a broad scope, ranging from basic support to highly technical care involving intravenous lines, ventilators, portable diagnostic tests, and remote monitors.4 Patients cared for at home range from those who are ambulatory to those who are permanently bedfast and seriously ill. The home care user population can be categorized based on the types of health care resources they consume (Table 1). Much attention has been paid to home-based care during recuperation after acute illness. The aim has been to foster recovery and prevent further need for institutional care. Lately the term transitional care has been used in this context.
TRANSITIONAL CARE
Transitional care has long been a priority for visiting nurse agencies. In 1965, Medicare Part A, building from the tradition of urban parish nursing services, created an interdisciplinary industry. Medicare now certifies more than 10,000 agencies with more than 250,000 professional staff.5 For several reasons, beginning in the 1970s, US physicians have become less integrated into in-home care. Despite this and the challenge of managing medically complex patients with minimal active physician involvement, home health agencies provide a vital service. Further, they have demonstrated improved outcomes and cost savings.
Transitional care refers to specialized, short-term care for selected high-risk patients after an acute illness. The original objective of transitional care was to reduce hospital readmissions. Tested models include an approach developed by Coleman et al,6 based on four pillars: assistance with medication self-management, patient-centered and -owned medical record, timely follow-up with primary or specialty care, and “red flags” that indicate a worsening condition. This model, which yielded one-third fewer hospital readmissions and a savings of about $500 per patient in 6 months, is being adopted in many locations nationally.
Naylor and colleagues7,8 collaborated with hospital-based nurse practitioners (NPs) for 2 decades on a more intensive model. In the Naylor model, the NPs form a health care bridge from hospital to home for 4 weeks after hospital care and add an active medical care component to the home care team. Naylor et al7 reported a 50% reduction in the rehospitalization rate and a cost savings of approximately $3,000 per patient over 24 weeks. Naylor’s team observed these results among frail, elderly patients with a variety of conditions and comorbidities. The 2010 federal health care reform law as well as state and private insurer initiatives now encourage use of this and other integrated care models.
In a national demonstration program using performance improvement methods and careful data collection, 73 US home health agencies improved targeted clinical outcomes and reduced hospitalizations from baseline rates by approximately 7% within 3 to 4 years.9 The study included approximately 158,000 patients in the intervention group and 249,000 in the comparison group. However, in general the success demonstrated in this study has not been reflected nationally, and home health agencies have been weakly integrated with the remainder of the health care delivery system.
Medicare home health agency care has evolved rapidly in the past 15 years, with reporting of numerous quality measures that has created direct accountability of physicians to the public. Until as recently as the 1990s, many important measures of quality in medicine were available only to physicians and physician and hospital organizations through governmental and, in some cases, legal routes. This new quality-based accountability, along with fiscal pressure to reduce lengths of stay and to limit visits under prospective payment, are among the changes that are transforming the home health industry.